



HIV and STIs
The majority of HIV infections are sexually transmitted or are associated with pregnancy, childbirth and breastfeeding. Our work links prevention with treatment, care and support, reduces HIV-related stigma and discrimination, and responds to unique regional and national characteristics of the epidemic.
Articles by HIV and STIs

End gender based violence and HIV to ensure equity
18 July, Durban: Gender Based Violence (GBV) must be recognised and addressed if we are to end HIV and AIDS urged the International Planned Parenthood Federation (IPPF) and the United Nations Entity for Gender Equality and the Empowerment of Women (UN Women) at a panel during the International AIDS Conference Monday. The impact of HIV among women and girls in all their diversity is significant and alarming. Women’s greater physical vulnerability to HIV is compounded by social norms, gender inequalities, poverty and violence. Women living with HIV are also more likely to face stigmatisation, infertility, and even abuse and abandonment, contributing to their disempowerment. In East and Southern Africa, the risk of HIV among women who have experienced violence maybe three times higher In Uganda and South Africa studies found women who experienced intimate partner violence were 50 per cent more likely to have HIV than women who had not experienced violence. In many countries in Africa, getting married is among the ‘riskiest’ behaviour for women, where they may be exposed to unprotected sex with a husband who has multiple sexual partners, and to underlying power dynamics between men and women that prevent women from accessing condoms and then insisting on their use. Julia Omondi, a 24 year old advocate from Family Health Options Kenya (FHOK) highlighted the most common root causes of gender based violence and HIV, ‘I work with a group of 50 young girls like myself, called the 3E advocates to prevent girls from child marriage; support girls who are living with HIV to understand their rights, make parents and communities aware of the laws that protect girls from child marriage. We need to raise our voices to stop child marriage and turn the tide against HIV’. “Empowerment + Engagement = Equality” is a joint project supported by UN Women and IPPF implemented in Kenya, Malawi and Uganda to address HIV vulnerability among adolescent girls and young women by engaging and empowering them. Traditional leaders like the senior chief Theresa Kachindamoto from Malawi spoke of her role to change harmful gender related practices, she said, ‘Chiefs as custodians of culture should be at the forefront to end cultural practices that negatively affect people’s health like sexual cleansing (Fisi), chief blanket. My village is now a model for others and my fellow chiefs come to learn about the change I have brought to Dedtza district in Malawi.’ Nazneen Damji, Policy Advisor- gender equality, health and HIV/AIDS at UN Women, highlighted the recognition by global leaders on the importance of addressing GBV and HIV. “Violence, and the fear of violence, can play a major role in women’s reluctance to know her HIV status and seek care. Fortunately, the Political Declaration on HIV/AIDS adopted in June at the UN General Assembly and the Resolution on women, the girl child and HIV adopted at the 60th Session of the Commission on the Status of Women both call on governments to intensify efforts to end all forms of violence against women and girls, including harmful practices that contribute to the spread of HIV amongst women and girls” ‘Civil society organisations like IPPF play an important part in holding governments accountable. We shouldn’t underestimate our role as advocates to inform national, regional and global policies. If we are to address the dual epidemics of GBV and HIV we need to have progressive polices where perpetrators can be brought to justice and laws and policies uphold gender equality’ said Zelda Nhlabatsi, the executive director of Family Life Association of Swaziland (FLAS). The session was sponsored by IPPF Africa Region, UN Women and the Ford Foundation.
14 July 2016
Sexual health and education in the slums: one year in Kibera
Lorraine Nabwire has a hard job, in a tough place. Lorraine is centre manager of the Family Health Options Kenya (FHOK) clinic in Kibera, Nairobi – a place best known for being Africa’s biggest urban slum. No-one is sure exactly how many people live crammed into Kibera – estimates range from fewer than 200,000 to around 800,000. But there’s no doubting the challenges faced by its residents. “Poverty here is high, people are poor,” explains Lorraine. “People do not have flushing toilets; they share latrines, maybe one for five families. When it rains they flood into the roads. And the drains are open. They pose a risk to children and it’s why we have a lot of cholera in Kibera.” Homes in Kibera are invariably tiny corrugated iron shacks, with mud or concrete walls, one crammed by the next. Running water comes from shared standpipes. Electricity is hooked illegally, and dangerously, from power lines. “When the power company removes them they just come back. The poor connections for electricity mean we have a lot of fires here,” Lorraine says. Until 2015, FHOK provided sexual health care in Kibera from mobile units. Then in July, a permanent centre was opened. Lorraine has been in charge of it since day one. Amid the shanties, the FHOK clinic in Kibera is a welcoming place; brightly painted outside with a mural showing a carefully planned, smiling family, cool and calm inside. But to walk inside involves stepping over an open drain – a reminder of its whereabouts. Lorraine is very honest about the challenges she has encountered in Kibera. “It’s work in progress. At the start we might get five people a day coming to us. Now it is more than 20. It’s good to be positive, despite progress being slow.” It’s clear there is a great need for better sexual health care in Kibera. “People in Kibera do have many children, and the child bearing age is early, as early as 15,” explains Lorraine. “By the time they are 24 they have four kids, or more.” Backstreet abortions are frequent, and HIV infection and rates of sexually transmitted infections (STIs) are also a concern. But despite the unmet need for sexual health services and the low cost of treatment – most tests are no more than 50 Kenyan Shillings, about half a US dollar, and even those fees are waived for people who can’t pay at all - worries about stigma and myths around the side effects of family planning discourages potential clients. “The young, say 15 to 19, have fear of being stigmatised. They think someone might say “Hey, you?” so they don’t come. There is poor health-seeking among the youth, but also an unmet need for family planning,” explains Lorraine. Myths around family planning are also a problem. “People think family planning causes infertility, causes bleeding in pregnancy and other things. Most of these comments come from men, but if they do not want women to come they will not.” Changing attitudes is very much part of the work of Lorraine’s team, and they have developed a battery of methods. “We recruited community health volunteers in Kibera, our voice and our ears,” says Lorraine. “They refer people who need our services to us, tell us what people are saying about us and what they need that we are not giving. Since then our client flow has been improving. We had an in-reach day recently and we had about 80 clients. That was good.” Lorraine and her staff also take part in a weekly radio show, called “Health Talk” on the local Swahili radio station to challenge stigma and myths. Regular community events are helping, and the team also goes into schools in Kibera to teach sexuality education. “Sexual debut is as early as nine, so we are going into primary schools as well as secondary schools,” Lorraine says. “If you don’t start until children are 14 then you are already late.” As the FHOK clinic in Kibera celebrates its first anniversary, Lorraine is clear about how she hopes it will develop in the year ahead. “I want to see the community taking-up what we are doing so that it is community-led, not FHOK-led, so we are behind the scenes. We have to be part of the community.”
30 June 2016
Girls Decide
This programme addresses critical challenges faced by young women around sexual health and sexuality. It has produced a range of advocacy, education and informational materials to support research, awareness-raising, advocacy and service delivery. Girls Decide is about the sexual and reproductive health and rights of girls and young women. Around the world, girls aged 10 to 19 account for 23% of all disease associated with pregnancy and childbirth. An estimated 2.5 million have unsafe abortions every year. Worldwide, young women account for 60% of the 5.5 million young people living with HIV and/or AIDS. Girls Decide has produced a range of advocacy, education and informational materials to support work to improve sexual health and rights for girls and young women. These include a series of films on sexual and reproductive health decisions faced by 6 young women in 6 different countries. The films won the prestigious International Video and Communications Award (IVCA). When girls and young women have access to critical lifesaving services and information, and when they are able to make meaningful choices about their life path, they are empowered. Their quality of life improves, as does the well-being of their families and the communities in which they live. Their collective ability to achieve internationally agreed development goals is strengthened. Almost all IPPF Member Associations provide services to young people and 1 in every 3 clients is a young person below the age of 25. All young women and girls are rights-holders and are entitled to sexual and reproductive rights. As a matter of principle, the IPPF Secretariat and Member Associations stand by girls by respecting and fulfilling their right to high quality services; they stand up for girls by supporting them in making their own decisions related to sexuality and pregnancy; they stand for sexual and reproductive rights by addressing the challenges faced by young women and girls at local, national and international levels.
22 June 2016
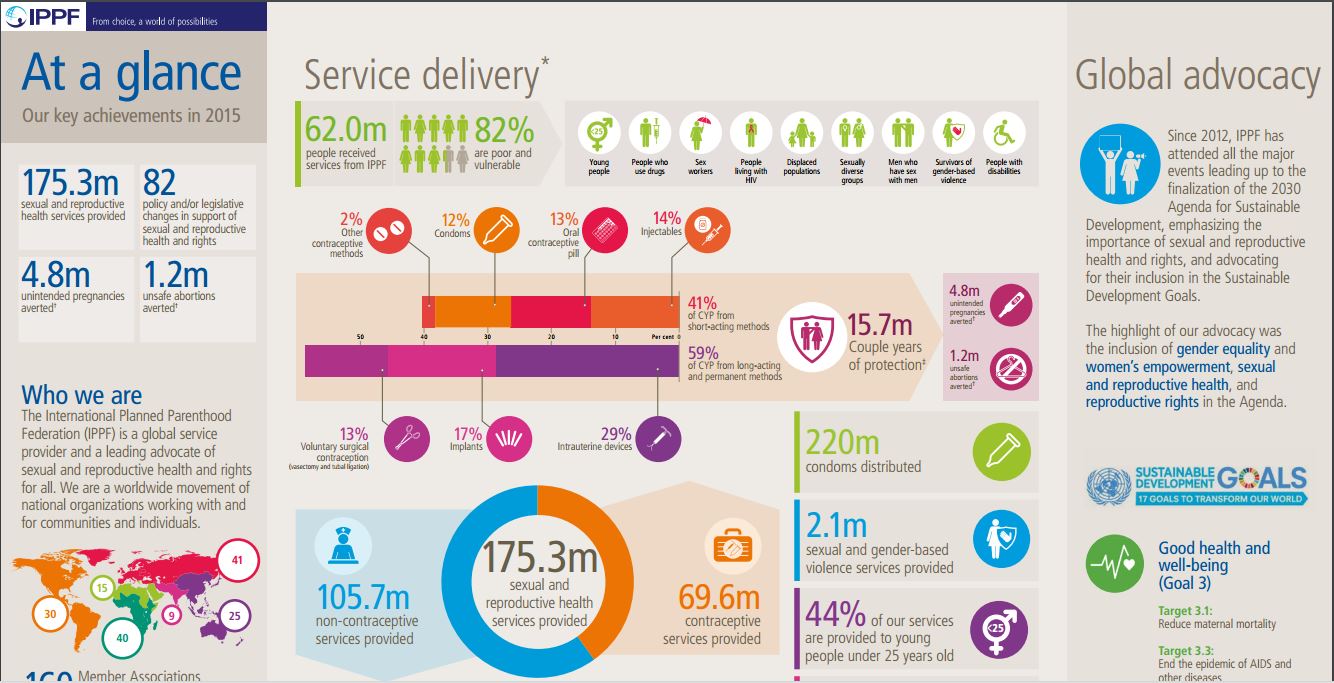
At a Glance 2015
Key facts and figures highlighting IPPF's achievements in 2015.

16 June 2016
Service Delivery
Women and girls around the world have an unmet need for reproductive health services. In 2015, IPPF provided 175 million services, 82% of which went to poor and marginalised people.
31 May 2015
Sexual and reproductive health and rights are the key to gender equality and sustainable development
Kate Gilmore, UNFPA Deputy Executive Director (Programme) addressed our High Level Side Event “Sexual and Reproductive Health and Rights: The key to gender equality and the empowerment of women and girls” at the 59th Commission on the Status of Women. Upholding human rights for sexual and reproductive health is key to ensuring that all people can be equal and free to make decisions in all spheres of their lives, without discrimination, without violence or coercion, and with the assurance of their dignity upheld. Together the outcomes of the Vienna human rights conference (1993) affirming indivisibility and universality of human rights, the Cairo population and development conference (1994) putting the person at the centre of development and the Beijing women’s conference (1995) affirming that women’s rights are indeed human rights, set a complimentary agenda – defined by the international community and reaffirmed globally time and time again. This is the agenda by which rights in respect of sexual and reproductive health are made normative and the means by which these rights are to be protected universally. It is on this foundation that women and girls, in particular, are reliant if they are to enjoy a life of choices, empowerment and equality, and this invokes the right to health throughout the life course inclusive of the right to make choices freely in marriage, family formation and determination of the number, timing and spacing of children. For such rights to be exercised and enjoyed, people – and women and young people in particular - must be supported with quality access to information, to services and to the means by which to exercise their voluntary choices. SRHR are rights in principle, upheld by international and universal norms and supported indivisibly, by all other human rights norms. However, they are also rights that, in practice, save lives and reduce ill-health: If all pregnant women and their newborns were to receive care at WHO recommended standards, if all women who want to avoid a an unplanned pregnancy had access to modern contraceptives, the life-saving benefits would be substantial. Maternal deaths would drop by 67%. Newborn deaths would drop by 77%. Unintended pregnancies would drop by 70%. Women’s and newborns’ burden of disability related to pregnancy and childbirth would drop by 66%. Transmission of HIV from mothers to newborns would be nearly eliminated—a 93% reduction. The correct thing to do in principle, upholding SRHR is just smart in practice. At its simplest, universal access to sexual and reproductive health is cost effective. With far fewer unintended pregnancies, the costs of improving pregnancy-, birth- and newborn-care, and of preventing mother-to-child transmission of HIV, are lowered. For each dollar spent on contraceptive services, the cost of pregnancy-related care reduces by $1.47. Expanding access to modern methods of contraception, and associated services, so that current rates of unmet need are met, would result in 163,000 fewer infants infected with HIV by 2015, while reducing total HIV treatment costs by $200 million. The UNFPA and the Guttmacher Institute report Adding It Up calculates that to provide essential sexual and reproductive health services to all women and girls aged 15-49 in developing countries would cost a mere $25 per woman per year, which, incidentally, is the cost of a movie ticket with popcorn in New York city. When human rights in sexual and reproductive health are upheld total claims on a country’s health budget are reduced while economic productivity and growth are stimulated; promoting a demographic transition that boosts both economic growth and individual wellbeing. When the number of dependent children in a country decreases, the ratio of productive workers to dependents increases, driving faster economic growth and reducing burdens on families. This window of opportunity is known as a ‘demographic dividend’ and with more young people than ever before this promises both a “youth” and a “gender” dividend, generating broader, long-term benefits for women, young people, their children, partners and families, economies and societies. Preventing maternal deaths and disability also helps protect individuals and families from catastrophic health expenses and loss of income while preventing unintended pregnancy reduces poverty by increasing women’s and girls’ ability to both access education and employment opportunities and participate more fully in social, political and economic life. A study conducted in 2013 in Kenya shows that families experiencing a maternal death spend more on medical care and funeral expenses than all other yearly expenses combined, including food, shelter, and education. The impact of complications of unsafe abortion and the expense of treating these are also substantial for households. Human rights associated with sexual and reproductive health matter for women’s economic, educational, and political empowerment and thus for their countries’ advance too. The autonomy to decide whether, when and with whom to have children, and the opportunity to access quality health services whenever and wherever she needs, is essential to the realization of her other life opportunities and fulfilment. These realities underscore why the promotion and protection of rights pertaining to sexual and reproductive health are instrumental to the achievement of all human rights including the right to education, the right to decent work, the right to food and the right to participation. While sexual and reproductive health are human rights in principle, they are also right the thing to do strategically and thus right in practice. Yet, still many women and girls around the world are denied exercise of their rights. Therefore tackling harmful gender norms is a must, given they are at the core of why so many women and girls are deprived of their rights to sexual and reproductive health. Female genital mutilation, child marriage, rape in marriage, wife inheritance and maltreatment of widows and son preference are all forms of gender based violence and each constitutes a grave impediment to the realization of human rights intrinsic to sexual and reproductive health. At the same time, unless the grave discrimination and inequalities faced by specific population groups are addressed (i.e. those faced by adolescent girls, persons with disabilities, indigenous women and girls, persons living with HIV, displaced persons, the elderly, LGBT, sex workers and others) we will continue to leave millions of people far behind the sustainable development agenda. Nowhere is this clearer than in regards to adolescents and young person. Today’s youth are 1.8 billion strong, forming a quarter of the world’s population. They are shaping social and economic development, challenging social norms and values, and setting the terms of the world’s future. While notable progress has been made under the Millennium Development Goals, many young people – especially adolescent girls – are still denied the investments and opportunities that they require to realize their full potential. Instead, for millions of girl children around the world, puberty – the biological onset of adolescence – brings not only often incomprehensible changes to their bodies but – thanks to perverse gender norms – also new vulnerabilities to human rights abuses, particularly in the arenas of sexuality, marriage and child bearing. The Beijing+20 review has highlighted that in the past 20 years much has been achieved. Increasingly countries are removing discrimination from their laws and adopting laws to promote gender equality and address violence against women and girls. There have been significant gains in girls’ enrolment in primary and – to some extent – in secondary education too. In some regions, women’s participation in the labour force has increased while some regions have made remarkable progress in increasing women’s access to contraception. There have been important gains in women’s representation in national parliaments and significant normative advances have been won in the global agenda on women, peace and security. However, 20 years on from Beijing, we can see what for women amounts to a life-threatening disconnect between agreed normative frameworks and the reality on the ground. Implementation, accountability and engaged must be strengthened. Without strong accountability mechanisms to enable women to hold decision makers answerable for their actions, substantial progress for human rights in sexual and reproductive health is unlikely. To turn this around, commensurate financial resources and political support for key institutions and mechanisms that promote gender equality, and the human rights of women and girls more broadly is essential, including for such as national gender equality mechanisms and national human rights institutions. Ensuring there are mechanisms for tracking and reporting on commitments made to human rights in sexual and reproductive health is also an essential part of building and fortifying accountability. UNFPA is undertaking bold and innovative measures to turn advance human rights. We are supporting countries to address gender and sexual based violence, for example, by working with sister UN agencies to support governments provide access to essential services for survivors and victims of gender based violence. We are enabling South-South cooperation and learning between countries through ground-breaking initiatives like the VIRAVIDA programme in Brazil, which brings together the private sector, government and community organizations to empower, educate and employ marginalized young people who have been sexually violated. By committing resources and action to support women and girls around the world to exercise autonomy over their bodies and fertility, including by enabling access to safe, voluntary family planning, we are ensuring realization of rights pertaining to their education and their labour force participation. Promoting the engagement of men as supportive partners in gender equality, we have established “husbands’ schools” that aim to promote better health for women and children. Implementing our Adolescent Girls Initiative, we are reaching the most marginalized adolescent girls, protecting their rights, particularly by delaying age at marriage and childbearing, by empowering them and by elevating their social status in their communities. Right in principle, smart in practice and plain strategic for sustainable development: the most pressing question cannot be “why should governments invest in human rights for sexual and reproductive health?” but rather “why haven’t they?”

Webinar: Addressing SRH and HIV needs among transgender people
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: Transgender people - The case of India” took place on Thursday, 26 March 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar is part of a series highlighting the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session will focus on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars will be held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. This first webinar focussed on “Transgender People: The Case of India”. Besides highlighting the importance of SRH and HIV linkages including integrated service provision for transgender people, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations; discuss the main barriers and challenges transgender people face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included JoAnne Keatly from the Center of Excellence for Transgender Health and Nisha Jagdish from the Family Planning Association of India. The presentation slides are available to download.

Webinar: Addressing SRH and HIV needs among sex workers
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: Sex workers - the case of Uganda” took place on Thursday, 18 June 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar series is highlighting the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session will focus on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars will be held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. The first webinar was held on 26 March: “Transgender People: The Case of India”. The second webinar focussed on “Sex Workers: The Case of Uganda”. Besides highlighting the importance of SRH and HIV linkages including integrated service provision for sex workers, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations, and the Sex Worker Implementation Tool (SWIT); discuss the main barriers and challenges sex workers face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included Anlina Sheng from the Global Network of Sex Work Projects (NSWP), Denis Bakomeza from Reproductive Health Uganda (RHU), and Ed Ngoksin from The Global Fund to Fight AIDS, Tuberculosis and Malaria. The presentation slides are available to download.

Webinar: Addressing SRH and HIV needs among people who use drugs
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: People who use drugs - the case of Kenya” took place on Thursday, 27 August 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar series is highlighting the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session focuses on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars are held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. The first webinar was held on 26 March: “Transgender People: The Case of India”; and the second webinar was held on 18 June: “Sex Workers: The Case of Uganda”. This third webinar focussed on "People who use drugs: The Case of Kenya". Besides highlighting the importance of SRH and HIV linkages including integrated service provision for people, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations; discuss the main barriers and challenges people who use drugs face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included Ruth Birgin from the International Network of People who use Drugs (INPUD), Lilian Kayaro from Family Health Option Kenya (FHOK), and Mauro Guarinieri from The Global Fund to Fight AIDS, Tuberculosis and Malaria. Background about Kenya: In Kenya the HIV epidemic has high prevalence among key populations including people who use drugs. There are clear indications of both rapid increases of drug use and HIV prevalence amongst this community, which was reported as 18% in 2011 (UNAIDS 2012). Government services are seeking to respond to this through the recent introduction of harm reduction interventions. These however face opposition from conservative and religious groups within Kenya, illustrating the stigma these populations face, and corresponding barriers to service access. Family Health Options Kenya (FHOK) have clinic sites in coastal areas of Kenya where this concentrated HIV epidemic is focussed, and so well placed to respond. In this first year implementing period, FHOK commenced the project with orientation meetings for the staff team both at Head Office and at the Coast Region Office and clinic. The project is building on a call for community partnership to increase access to harm reduction counselling and support for people who use drugs. The presentation slides are available to download.

Webinar: Addressing SRH and HIV needs among men who have sex with men
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: Men who have sex with men - the case of Cameroon” took place on Thursday, 15 October 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar series highlighted the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session focuses on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars are held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. The first webinar was held on 26 March: “Transgender People: The Case of India”; the second webinar was held on 18 June: “Sex Workers: The Case of Uganda”, and the third webinar focussed on "People who use drugs: The Case of Kenya" on 27 August. This fourth webinar focussed on "Men who have sex with men - the case of Cameroon". Besides highlighting the importance of SRH and HIV linkages including integrated service provision for people, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations; discuss the main barriers and challenges people who use drugs face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included Sonya Arreola from the Global Forum on MSM and HIV (MSMGF), Arouna Tena from the Cameroon National Association for Family Welfare (CAMNAFAW), and Ed Ngoksin from The Global Fund to Fight AIDS, Tuberculosis and Malaria. Background about Cameroon: In Cameroon, the SRH and HIV service needs of MSM are largely ignored. Owing to the political sensitivity of this issue, NGOs and leaders of national programmes do not often adapt their programmes and do not create an enabling environment for action. Discrimination from health service providers and a lack of sexual health information leave people of diverse sexual orientations and gender identities vulnerable to poor health. One of the consequences of this situation is a high HIV and STI prevalence among MSM. As a principal recipient under the Global Fund project, CAMNAFAW is contributing to the strategy to reduce the transmission of HIV among ‘most-at-risk populations’. CAMNAFAW in collaboration with other principal recipients are identifying the current gaps, with a focus on providing services to MSM and the wider LGBTI community in Yaoundé and Douala. The presentation slides are available to download.
End gender based violence and HIV to ensure equity
18 July, Durban: Gender Based Violence (GBV) must be recognised and addressed if we are to end HIV and AIDS urged the International Planned Parenthood Federation (IPPF) and the United Nations Entity for Gender Equality and the Empowerment of Women (UN Women) at a panel during the International AIDS Conference Monday. The impact of HIV among women and girls in all their diversity is significant and alarming. Women’s greater physical vulnerability to HIV is compounded by social norms, gender inequalities, poverty and violence. Women living with HIV are also more likely to face stigmatisation, infertility, and even abuse and abandonment, contributing to their disempowerment. In East and Southern Africa, the risk of HIV among women who have experienced violence maybe three times higher In Uganda and South Africa studies found women who experienced intimate partner violence were 50 per cent more likely to have HIV than women who had not experienced violence. In many countries in Africa, getting married is among the ‘riskiest’ behaviour for women, where they may be exposed to unprotected sex with a husband who has multiple sexual partners, and to underlying power dynamics between men and women that prevent women from accessing condoms and then insisting on their use. Julia Omondi, a 24 year old advocate from Family Health Options Kenya (FHOK) highlighted the most common root causes of gender based violence and HIV, ‘I work with a group of 50 young girls like myself, called the 3E advocates to prevent girls from child marriage; support girls who are living with HIV to understand their rights, make parents and communities aware of the laws that protect girls from child marriage. We need to raise our voices to stop child marriage and turn the tide against HIV’. “Empowerment + Engagement = Equality” is a joint project supported by UN Women and IPPF implemented in Kenya, Malawi and Uganda to address HIV vulnerability among adolescent girls and young women by engaging and empowering them. Traditional leaders like the senior chief Theresa Kachindamoto from Malawi spoke of her role to change harmful gender related practices, she said, ‘Chiefs as custodians of culture should be at the forefront to end cultural practices that negatively affect people’s health like sexual cleansing (Fisi), chief blanket. My village is now a model for others and my fellow chiefs come to learn about the change I have brought to Dedtza district in Malawi.’ Nazneen Damji, Policy Advisor- gender equality, health and HIV/AIDS at UN Women, highlighted the recognition by global leaders on the importance of addressing GBV and HIV. “Violence, and the fear of violence, can play a major role in women’s reluctance to know her HIV status and seek care. Fortunately, the Political Declaration on HIV/AIDS adopted in June at the UN General Assembly and the Resolution on women, the girl child and HIV adopted at the 60th Session of the Commission on the Status of Women both call on governments to intensify efforts to end all forms of violence against women and girls, including harmful practices that contribute to the spread of HIV amongst women and girls” ‘Civil society organisations like IPPF play an important part in holding governments accountable. We shouldn’t underestimate our role as advocates to inform national, regional and global policies. If we are to address the dual epidemics of GBV and HIV we need to have progressive polices where perpetrators can be brought to justice and laws and policies uphold gender equality’ said Zelda Nhlabatsi, the executive director of Family Life Association of Swaziland (FLAS). The session was sponsored by IPPF Africa Region, UN Women and the Ford Foundation.
14 July 2016
Sexual health and education in the slums: one year in Kibera
Lorraine Nabwire has a hard job, in a tough place. Lorraine is centre manager of the Family Health Options Kenya (FHOK) clinic in Kibera, Nairobi – a place best known for being Africa’s biggest urban slum. No-one is sure exactly how many people live crammed into Kibera – estimates range from fewer than 200,000 to around 800,000. But there’s no doubting the challenges faced by its residents. “Poverty here is high, people are poor,” explains Lorraine. “People do not have flushing toilets; they share latrines, maybe one for five families. When it rains they flood into the roads. And the drains are open. They pose a risk to children and it’s why we have a lot of cholera in Kibera.” Homes in Kibera are invariably tiny corrugated iron shacks, with mud or concrete walls, one crammed by the next. Running water comes from shared standpipes. Electricity is hooked illegally, and dangerously, from power lines. “When the power company removes them they just come back. The poor connections for electricity mean we have a lot of fires here,” Lorraine says. Until 2015, FHOK provided sexual health care in Kibera from mobile units. Then in July, a permanent centre was opened. Lorraine has been in charge of it since day one. Amid the shanties, the FHOK clinic in Kibera is a welcoming place; brightly painted outside with a mural showing a carefully planned, smiling family, cool and calm inside. But to walk inside involves stepping over an open drain – a reminder of its whereabouts. Lorraine is very honest about the challenges she has encountered in Kibera. “It’s work in progress. At the start we might get five people a day coming to us. Now it is more than 20. It’s good to be positive, despite progress being slow.” It’s clear there is a great need for better sexual health care in Kibera. “People in Kibera do have many children, and the child bearing age is early, as early as 15,” explains Lorraine. “By the time they are 24 they have four kids, or more.” Backstreet abortions are frequent, and HIV infection and rates of sexually transmitted infections (STIs) are also a concern. But despite the unmet need for sexual health services and the low cost of treatment – most tests are no more than 50 Kenyan Shillings, about half a US dollar, and even those fees are waived for people who can’t pay at all - worries about stigma and myths around the side effects of family planning discourages potential clients. “The young, say 15 to 19, have fear of being stigmatised. They think someone might say “Hey, you?” so they don’t come. There is poor health-seeking among the youth, but also an unmet need for family planning,” explains Lorraine. Myths around family planning are also a problem. “People think family planning causes infertility, causes bleeding in pregnancy and other things. Most of these comments come from men, but if they do not want women to come they will not.” Changing attitudes is very much part of the work of Lorraine’s team, and they have developed a battery of methods. “We recruited community health volunteers in Kibera, our voice and our ears,” says Lorraine. “They refer people who need our services to us, tell us what people are saying about us and what they need that we are not giving. Since then our client flow has been improving. We had an in-reach day recently and we had about 80 clients. That was good.” Lorraine and her staff also take part in a weekly radio show, called “Health Talk” on the local Swahili radio station to challenge stigma and myths. Regular community events are helping, and the team also goes into schools in Kibera to teach sexuality education. “Sexual debut is as early as nine, so we are going into primary schools as well as secondary schools,” Lorraine says. “If you don’t start until children are 14 then you are already late.” As the FHOK clinic in Kibera celebrates its first anniversary, Lorraine is clear about how she hopes it will develop in the year ahead. “I want to see the community taking-up what we are doing so that it is community-led, not FHOK-led, so we are behind the scenes. We have to be part of the community.”
30 June 2016
Girls Decide
This programme addresses critical challenges faced by young women around sexual health and sexuality. It has produced a range of advocacy, education and informational materials to support research, awareness-raising, advocacy and service delivery. Girls Decide is about the sexual and reproductive health and rights of girls and young women. Around the world, girls aged 10 to 19 account for 23% of all disease associated with pregnancy and childbirth. An estimated 2.5 million have unsafe abortions every year. Worldwide, young women account for 60% of the 5.5 million young people living with HIV and/or AIDS. Girls Decide has produced a range of advocacy, education and informational materials to support work to improve sexual health and rights for girls and young women. These include a series of films on sexual and reproductive health decisions faced by 6 young women in 6 different countries. The films won the prestigious International Video and Communications Award (IVCA). When girls and young women have access to critical lifesaving services and information, and when they are able to make meaningful choices about their life path, they are empowered. Their quality of life improves, as does the well-being of their families and the communities in which they live. Their collective ability to achieve internationally agreed development goals is strengthened. Almost all IPPF Member Associations provide services to young people and 1 in every 3 clients is a young person below the age of 25. All young women and girls are rights-holders and are entitled to sexual and reproductive rights. As a matter of principle, the IPPF Secretariat and Member Associations stand by girls by respecting and fulfilling their right to high quality services; they stand up for girls by supporting them in making their own decisions related to sexuality and pregnancy; they stand for sexual and reproductive rights by addressing the challenges faced by young women and girls at local, national and international levels.
22 June 2016
At a Glance 2015
Key facts and figures highlighting IPPF's achievements in 2015.
16 June 2016
Service Delivery
Women and girls around the world have an unmet need for reproductive health services. In 2015, IPPF provided 175 million services, 82% of which went to poor and marginalised people.
31 May 2015
Sexual and reproductive health and rights are the key to gender equality and sustainable development
Kate Gilmore, UNFPA Deputy Executive Director (Programme) addressed our High Level Side Event “Sexual and Reproductive Health and Rights: The key to gender equality and the empowerment of women and girls” at the 59th Commission on the Status of Women. Upholding human rights for sexual and reproductive health is key to ensuring that all people can be equal and free to make decisions in all spheres of their lives, without discrimination, without violence or coercion, and with the assurance of their dignity upheld. Together the outcomes of the Vienna human rights conference (1993) affirming indivisibility and universality of human rights, the Cairo population and development conference (1994) putting the person at the centre of development and the Beijing women’s conference (1995) affirming that women’s rights are indeed human rights, set a complimentary agenda – defined by the international community and reaffirmed globally time and time again. This is the agenda by which rights in respect of sexual and reproductive health are made normative and the means by which these rights are to be protected universally. It is on this foundation that women and girls, in particular, are reliant if they are to enjoy a life of choices, empowerment and equality, and this invokes the right to health throughout the life course inclusive of the right to make choices freely in marriage, family formation and determination of the number, timing and spacing of children. For such rights to be exercised and enjoyed, people – and women and young people in particular - must be supported with quality access to information, to services and to the means by which to exercise their voluntary choices. SRHR are rights in principle, upheld by international and universal norms and supported indivisibly, by all other human rights norms. However, they are also rights that, in practice, save lives and reduce ill-health: If all pregnant women and their newborns were to receive care at WHO recommended standards, if all women who want to avoid a an unplanned pregnancy had access to modern contraceptives, the life-saving benefits would be substantial. Maternal deaths would drop by 67%. Newborn deaths would drop by 77%. Unintended pregnancies would drop by 70%. Women’s and newborns’ burden of disability related to pregnancy and childbirth would drop by 66%. Transmission of HIV from mothers to newborns would be nearly eliminated—a 93% reduction. The correct thing to do in principle, upholding SRHR is just smart in practice. At its simplest, universal access to sexual and reproductive health is cost effective. With far fewer unintended pregnancies, the costs of improving pregnancy-, birth- and newborn-care, and of preventing mother-to-child transmission of HIV, are lowered. For each dollar spent on contraceptive services, the cost of pregnancy-related care reduces by $1.47. Expanding access to modern methods of contraception, and associated services, so that current rates of unmet need are met, would result in 163,000 fewer infants infected with HIV by 2015, while reducing total HIV treatment costs by $200 million. The UNFPA and the Guttmacher Institute report Adding It Up calculates that to provide essential sexual and reproductive health services to all women and girls aged 15-49 in developing countries would cost a mere $25 per woman per year, which, incidentally, is the cost of a movie ticket with popcorn in New York city. When human rights in sexual and reproductive health are upheld total claims on a country’s health budget are reduced while economic productivity and growth are stimulated; promoting a demographic transition that boosts both economic growth and individual wellbeing. When the number of dependent children in a country decreases, the ratio of productive workers to dependents increases, driving faster economic growth and reducing burdens on families. This window of opportunity is known as a ‘demographic dividend’ and with more young people than ever before this promises both a “youth” and a “gender” dividend, generating broader, long-term benefits for women, young people, their children, partners and families, economies and societies. Preventing maternal deaths and disability also helps protect individuals and families from catastrophic health expenses and loss of income while preventing unintended pregnancy reduces poverty by increasing women’s and girls’ ability to both access education and employment opportunities and participate more fully in social, political and economic life. A study conducted in 2013 in Kenya shows that families experiencing a maternal death spend more on medical care and funeral expenses than all other yearly expenses combined, including food, shelter, and education. The impact of complications of unsafe abortion and the expense of treating these are also substantial for households. Human rights associated with sexual and reproductive health matter for women’s economic, educational, and political empowerment and thus for their countries’ advance too. The autonomy to decide whether, when and with whom to have children, and the opportunity to access quality health services whenever and wherever she needs, is essential to the realization of her other life opportunities and fulfilment. These realities underscore why the promotion and protection of rights pertaining to sexual and reproductive health are instrumental to the achievement of all human rights including the right to education, the right to decent work, the right to food and the right to participation. While sexual and reproductive health are human rights in principle, they are also right the thing to do strategically and thus right in practice. Yet, still many women and girls around the world are denied exercise of their rights. Therefore tackling harmful gender norms is a must, given they are at the core of why so many women and girls are deprived of their rights to sexual and reproductive health. Female genital mutilation, child marriage, rape in marriage, wife inheritance and maltreatment of widows and son preference are all forms of gender based violence and each constitutes a grave impediment to the realization of human rights intrinsic to sexual and reproductive health. At the same time, unless the grave discrimination and inequalities faced by specific population groups are addressed (i.e. those faced by adolescent girls, persons with disabilities, indigenous women and girls, persons living with HIV, displaced persons, the elderly, LGBT, sex workers and others) we will continue to leave millions of people far behind the sustainable development agenda. Nowhere is this clearer than in regards to adolescents and young person. Today’s youth are 1.8 billion strong, forming a quarter of the world’s population. They are shaping social and economic development, challenging social norms and values, and setting the terms of the world’s future. While notable progress has been made under the Millennium Development Goals, many young people – especially adolescent girls – are still denied the investments and opportunities that they require to realize their full potential. Instead, for millions of girl children around the world, puberty – the biological onset of adolescence – brings not only often incomprehensible changes to their bodies but – thanks to perverse gender norms – also new vulnerabilities to human rights abuses, particularly in the arenas of sexuality, marriage and child bearing. The Beijing+20 review has highlighted that in the past 20 years much has been achieved. Increasingly countries are removing discrimination from their laws and adopting laws to promote gender equality and address violence against women and girls. There have been significant gains in girls’ enrolment in primary and – to some extent – in secondary education too. In some regions, women’s participation in the labour force has increased while some regions have made remarkable progress in increasing women’s access to contraception. There have been important gains in women’s representation in national parliaments and significant normative advances have been won in the global agenda on women, peace and security. However, 20 years on from Beijing, we can see what for women amounts to a life-threatening disconnect between agreed normative frameworks and the reality on the ground. Implementation, accountability and engaged must be strengthened. Without strong accountability mechanisms to enable women to hold decision makers answerable for their actions, substantial progress for human rights in sexual and reproductive health is unlikely. To turn this around, commensurate financial resources and political support for key institutions and mechanisms that promote gender equality, and the human rights of women and girls more broadly is essential, including for such as national gender equality mechanisms and national human rights institutions. Ensuring there are mechanisms for tracking and reporting on commitments made to human rights in sexual and reproductive health is also an essential part of building and fortifying accountability. UNFPA is undertaking bold and innovative measures to turn advance human rights. We are supporting countries to address gender and sexual based violence, for example, by working with sister UN agencies to support governments provide access to essential services for survivors and victims of gender based violence. We are enabling South-South cooperation and learning between countries through ground-breaking initiatives like the VIRAVIDA programme in Brazil, which brings together the private sector, government and community organizations to empower, educate and employ marginalized young people who have been sexually violated. By committing resources and action to support women and girls around the world to exercise autonomy over their bodies and fertility, including by enabling access to safe, voluntary family planning, we are ensuring realization of rights pertaining to their education and their labour force participation. Promoting the engagement of men as supportive partners in gender equality, we have established “husbands’ schools” that aim to promote better health for women and children. Implementing our Adolescent Girls Initiative, we are reaching the most marginalized adolescent girls, protecting their rights, particularly by delaying age at marriage and childbearing, by empowering them and by elevating their social status in their communities. Right in principle, smart in practice and plain strategic for sustainable development: the most pressing question cannot be “why should governments invest in human rights for sexual and reproductive health?” but rather “why haven’t they?”
Webinar: Addressing SRH and HIV needs among transgender people
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: Transgender people - The case of India” took place on Thursday, 26 March 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar is part of a series highlighting the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session will focus on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars will be held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. This first webinar focussed on “Transgender People: The Case of India”. Besides highlighting the importance of SRH and HIV linkages including integrated service provision for transgender people, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations; discuss the main barriers and challenges transgender people face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included JoAnne Keatly from the Center of Excellence for Transgender Health and Nisha Jagdish from the Family Planning Association of India. The presentation slides are available to download.
Webinar: Addressing SRH and HIV needs among sex workers
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: Sex workers - the case of Uganda” took place on Thursday, 18 June 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar series is highlighting the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session will focus on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars will be held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. The first webinar was held on 26 March: “Transgender People: The Case of India”. The second webinar focussed on “Sex Workers: The Case of Uganda”. Besides highlighting the importance of SRH and HIV linkages including integrated service provision for sex workers, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations, and the Sex Worker Implementation Tool (SWIT); discuss the main barriers and challenges sex workers face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included Anlina Sheng from the Global Network of Sex Work Projects (NSWP), Denis Bakomeza from Reproductive Health Uganda (RHU), and Ed Ngoksin from The Global Fund to Fight AIDS, Tuberculosis and Malaria. The presentation slides are available to download.
Webinar: Addressing SRH and HIV needs among people who use drugs
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: People who use drugs - the case of Kenya” took place on Thursday, 27 August 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar series is highlighting the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session focuses on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars are held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. The first webinar was held on 26 March: “Transgender People: The Case of India”; and the second webinar was held on 18 June: “Sex Workers: The Case of Uganda”. This third webinar focussed on "People who use drugs: The Case of Kenya". Besides highlighting the importance of SRH and HIV linkages including integrated service provision for people, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations; discuss the main barriers and challenges people who use drugs face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included Ruth Birgin from the International Network of People who use Drugs (INPUD), Lilian Kayaro from Family Health Option Kenya (FHOK), and Mauro Guarinieri from The Global Fund to Fight AIDS, Tuberculosis and Malaria. Background about Kenya: In Kenya the HIV epidemic has high prevalence among key populations including people who use drugs. There are clear indications of both rapid increases of drug use and HIV prevalence amongst this community, which was reported as 18% in 2011 (UNAIDS 2012). Government services are seeking to respond to this through the recent introduction of harm reduction interventions. These however face opposition from conservative and religious groups within Kenya, illustrating the stigma these populations face, and corresponding barriers to service access. Family Health Options Kenya (FHOK) have clinic sites in coastal areas of Kenya where this concentrated HIV epidemic is focussed, and so well placed to respond. In this first year implementing period, FHOK commenced the project with orientation meetings for the staff team both at Head Office and at the Coast Region Office and clinic. The project is building on a call for community partnership to increase access to harm reduction counselling and support for people who use drugs. The presentation slides are available to download.
Webinar: Addressing SRH and HIV needs among men who have sex with men
“Addressing sexual and reproductive health (SRH) and HIV needs among key populations: Men who have sex with men - the case of Cameroon” took place on Thursday, 15 October 2015. The German BACKUP Initiative in collaboration with IPPF funded a three-year project, “Shadows and Light”, which addresses the sexual and reproductive health (SRH) and HIV needs of key populations at higher risk of HIV within four IPPF Member Associations (MAs). This included a focus on transgender people in India; sex workers in Uganda; people who use drugs in Kenya; and men who have sex with men in Cameroon. This webinar series highlighted the importance of addressing SRH within HIV programmes for key populations, and how Global Fund to fight AIDS, TB and Malaria (Global Fund) is integral to their success and sustainability. Each webinar session focuses on one key population. Facilitated by IPPF and the German BACKUP Initiative, the webinars are held in cooperation with key population networks or organizations; the Global Fund; and IPPF MAs. The first webinar was held on 26 March: “Transgender People: The Case of India”; the second webinar was held on 18 June: “Sex Workers: The Case of Uganda”, and the third webinar focussed on "People who use drugs: The Case of Kenya" on 27 August. This fourth webinar focussed on "Men who have sex with men - the case of Cameroon". Besides highlighting the importance of SRH and HIV linkages including integrated service provision for people, the webinar aimed to: introduce the SRH components of the consolidated WHO guidelines on HIV prevention, diagnosis, treatment and care for key populations; discuss the main barriers and challenges people who use drugs face to access SRH and HIV services; understand how addressing SRH within HIV programmes and services funded by the Global Fund is possible; and learn from country-level experiences about successful interventions, challenges and recommendations. Speakers included Sonya Arreola from the Global Forum on MSM and HIV (MSMGF), Arouna Tena from the Cameroon National Association for Family Welfare (CAMNAFAW), and Ed Ngoksin from The Global Fund to Fight AIDS, Tuberculosis and Malaria. Background about Cameroon: In Cameroon, the SRH and HIV service needs of MSM are largely ignored. Owing to the political sensitivity of this issue, NGOs and leaders of national programmes do not often adapt their programmes and do not create an enabling environment for action. Discrimination from health service providers and a lack of sexual health information leave people of diverse sexual orientations and gender identities vulnerable to poor health. One of the consequences of this situation is a high HIV and STI prevalence among MSM. As a principal recipient under the Global Fund project, CAMNAFAW is contributing to the strategy to reduce the transmission of HIV among ‘most-at-risk populations’. CAMNAFAW in collaboration with other principal recipients are identifying the current gaps, with a focus on providing services to MSM and the wider LGBTI community in Yaoundé and Douala. The presentation slides are available to download.