



Articles about Arab World

IPPF and Japan team up on another project to sustain sexual and reproductive health services in the West Bank, Palestine
21st April 2026 - IPPF and its Member Association in Palestine (PFPPA) are pleased to announce the launch of a new project financed by the Government of Japan, "Provision of health and medical services for women and children affected by crisis in the West Bank." This project will deliver life-saving maternal healthcare, psychosocial support, and sexual and reproductive health services, in even the hardest-to-reach areas of the West Bank, Palestine, through health centres, mobile medical teams, tele-consultations, and community outreach. The destruction of health facilities, severe restrictions on movement, and raids and attacks on communities in the West Bank have left Palestinians with little to no access to healthcare. According to the UNFPA, over 230,000 women and girls experience difficulties in accessing reproductive health services. Key project activities will include:Maintaining essential sexual and reproductive health (SRH) services, through three static clinics in Khalil, Halhoul and Bethlehem in the West Bank. These clinics will offer services including family planning, obstetrics and gynaecology care and management of sexually transmitted infections, for over 22,000 women and children. This will include specialised support for an estimated 2,300 survivors of sexual and gender-based violence, who will receive medical care, counselling or referrals. Providing maternal and child health care services for 4,600 women and children in hard-to-reach and marginalised areas of the West Bank via a mobile team of doctors, midwives, paediatricians, social workers, pharmacists and lab technicians. The mobile team will also provide psychosocial support services, support for survivors of sexual and gender-based violence, and family planning services. Providing counselling and consultation services via telecommunications and digital channels for those unable to access clinics.Conducting five ‘preparing for birth’ sessions for 90 first time mothers, providing information and support on maternal care and options for labour and delivery. Mr. ARAIKE Katsuhiko, Ambassador of Japan for the Palestinian Affairs says: “As a flagbearer of Universal Health Coverage (UHC) and the Women, Peace, and Security (WPS) agenda, we hope that our new collaboration with IPPF facilitates Palestinian women and children, who are affected by conflicts and live outside service catchment areas, to enjoy Obstetrics and Gynecology (OBGYN) and family planning services, improved well-being, and social participation. This project is part of Japan’s 2026–2027 cooperation package for Palestine. Japan will continue to provide support for the stability and prosperity of Palestine.” Dr. Fadoua Bakhadda, Regional Director of the IPPF Arab World Regional Office adds: “Thanks to the support of the people of Japan, we can continue delivering essential maternal and child health services to communities that have been systematically cut off from care, helping to prevent avoidable maternal and newborn deaths in the West Bank, Palestine.” -- About International Planned Parenthood Federation (IPPF) Arab World Office IPPF is a global healthcare provider and a leading advocate of sexual and reproductive health and rights (SRHR) for all. Led by a courageous and determined group of women, IPPF was founded in 1952. Today, we are a movement of over 120 autonomous member associations and 23 collaborative partners with a presence in 146 countries. Established in 1971, the IPPF Arab World Region (IPPF AWR) is one of IPPF’s six regional offices. Based in Tunis, it is the leading Sexual and Reproductive Health (SRH) service delivery organization in the North Africa and the Middle East, and the leading Sexual and Reproductive Health and Rights (SRHR) advocacy voice in the region.

Japan funds essential supplies for healthcare clinics in Sudan
16th April 2026 - A new project titled Strengthening Life-saving Sexual and Reproductive Health (SRH) Services for Internally Displaced Persons (IDPs), has been launched in Sudan. Funded by the Government of Japan and implemented by the IPPF Member Association Sudan Family Planning Association (SFPA), the project will support women and girls in crisis in the Red Sea and Khartoum States. Fifteen million people in Sudan have been displaced by the civil war, and conflicts in neighbouring countries have triggered an influx of returnees and displaced people into Sudan. As a result, the country now hosts 15% of the world’s IDPs. But widespread destruction of infrastructure and deadly disease outbreaks have left the healthcare system unable to cope.An estimated 1.75 million women and girls require urgent sexual and reproductive health (SRH) services, including 270,000 internally displaced pregnant women. With rape increasingly used as a weapon of war, many require urgent medical and psychosocial support. However, essential SRH commodities, including contraceptives, emergency obstetric kits, and menstrual hygiene products, are in critically low supply. SFPA provides essential sexual and reproductive health services to women and girls, including internally displaced persons, through 26 static clinics and 11 mobile clinics across the country. This new funding will enable them to procure, transport and distribute essential supplies to two of the organisation’s static clinics in the Red Sea State and Khartoum State. This vital equipment, including microscopes, blood-testing devices, thermometers, and examination lamps, will enable these clinics to continue providing SRH services, expanding their reach to an additional 2,400 internally displaced people and individuals in host communities. Mr. Nakahara Takanobu, the Chargé d’Affaires ad interim of the Embassy of Japan to Sudan, stated that, “The provision of sexual and reproductive healthcare for women and girls is a critical step in supporting this vulnerable category in Sudan. This is more so when they are IDPs. Thus, we are happy to be able to support IPPF’s Member Association in Sudan - the Sudan Family Planning Association - in this domain, so that we can contribute to improving the safety and well-being of these women and girls, and reassure them that we acknowledge the challenges they face and endure.” Dr Hiba Ahmed Khalil, Emergency and Humanitarian Interventions Manager at SFPA added, “SFPA is honoured to join the Japan Supplementary Budget 2025 project, advancing inclusive health and humanitarian responses that strengthen access to essential services and uphold the rights of communities most at risk. Together, we are building pathways for resilience and equity.” Dr. Fadoua Bakhadda, Regional Director of the IPPF Arab World Regional Office, added, “Every woman and girl deserves access to safe, reliable healthcare, no matter the circumstances. Thanks to the people of Japan, we can equip clinics with the essential tools and supplies needed to continue providing critical sexual and reproductive healthcare. This investment will directly improve the safety, health, and resilience of thousands of internally displaced women and girls.” ---About the Sudan Family Planning Association The Sudan Family Planning Association (SFPA) was established in 1965 by pioneers in obstetrics and gynaecology in response to increases in maternal, neonatal and infant mortality and morbidity. As the statistics show, Sudan is a country in great need of frontline sexual and reproductive health (SRH) services. Advocacy, and undertaking information, education and communication (IEC) programs are critical.About International Planned Parenthood Federation (IPPF) Arab World Office IPPF is a global healthcare provider and a leading advocate of sexual and reproductive health and rights (SRHR) for all. Led by a courageous and determined group of women, IPPF was founded in 1952. Today, we are a movement of over 120 autonomous member associations and 23 collaborative partners with a presence in 146 countries. Established in 1971, the IPPF Arab World Region (IPPF AWR) is one of IPPF’s six regional offices. Based in Tunis, it is the leading Sexual and Reproductive Health (SRH) service delivery organization in North Africa and the Middle East, and the leading Sexual and Reproductive Health and Rights (SRHR) advocacy voice in the region.

08 April 2026
IPPF Rejects the Instrumentalisation of human rights as a justification for war.
The bombing of Iran and the region by Israel and the United States is orchestrated by men who worship militarised masculinities and whose world views are founded on dominance, control, and aggression. These actions only serve their own power, and sustain systems of militarisation, imperialism and patriarchy under which women, girls, and marginalised communities disproportionality suffer. As the military assault against Iran by the US and Isreal intensifies on multiple fronts across the region, Donald Trump and Benjamin Netanyahu are using the same settler-colonial playbooks used in Gaza and further expanding it across the region. Under the pretext of “defending human rights”, Israel and the US are bombing densely populated areas and forcing entire communities to flee as a part of its strategy of colonial expansion and regional dominance.In Iran, mandatory veiling laws, criminalisation of abortion, restrictions on contraception, and the violent suppression of feminist activists is now being met with aerial bombardment. Women, girls, and marginalised communities are at the centre of a war between supremacists, where the dropping of bombs is the so-called precursor to peace and stability that takes the form of bombed clinics, decimated health systems, and burning oil infrastructure , which is blanketing Tehran in a toxic smoke that has lasting risks to maternal and reproductive health. In Lebanon, the destruction of infrastructure, road closures, and the constant threat of airstrikes are severely disrupting clinic activities and community health services. Many of those displaced are women and LGBTQI+ individuals who are pregnant, breastfeeding, or caring for newborns and young children, with nowhere safe to go. Overcrowded shelters often lack adequate sanitation, privacy, and basic supplies, undermining individuals' safety and mobility while heightening the risk of harassment, exploitation, and gender-based violence.All the while, the genocide in Gaza continues. Border crossings have been closed, movement in the West Bank has been shut down, and illegal settler and police violence continues whilst our attention is pulled to the multitude of crises at the hands of Donald Trump and Benjamin Netanyahu. The same ideological machismo that attacks bodily autonomy also glorifies war and destruction.The international community’s failure to stop the genocide in Gaza or enforce international humanitarian law, alongside the protection Israel receives from powerful allies, has emboldened this violence and enabled its expansion across the region and globally.The bombing and international interventions in Venezuela, Iran, Kurdistan-Iraq, Palestine, Nigeria, Somalia, Yemen and Syria, and now Lebanon, evidence how military power is being abused with no limits by the US. This use of force, bolstered by equally aggressive or compliant allies, is the new normal for the so called ‘President of Peace’.These are the same actors that are rolling back sexual and reproductive health, rights and justice (SRHRJ), and are simultaneously driving anti-LGBTQI+, and anti-migrant efforts in their own countries, while using the language of freedom to bomb others. This is matched by the scaffolding of white supremacy and a brand of masculinity that celebrates war and legitimises ultra conservative, traditionalist and illiberal leaders and authoritarian actors to leverage their foreign influence to weaken democratic norms and undermine regional security. All the while we draw on the language of a world order that is interpreted through a US and Global North centric lens, built by powerful states for powerful states on the coattails of patriarchy and colonialism. "The world we live in is designed by and for cisgender, straight men—a direct legacy of patriarchy. This same system creates and launches wars. Pregnant people, children, the elderly, and those living with disabilities or chronic illnesses are particularly vulnerable in these situations. Since caregiving is often an unpaid, unrecognized, and gendered task, women frequently bear the responsibility of caring for children and the elderly, often at the expense of their own health and needs. Furthermore, the mental health impact of war on women, girls, LGBTQIA+ individuals, and other marginalized communities remains an often overlooked issue." – Soudeh Rade, Executive Director, SpectrumBodily autonomy is not a separate issue – it is rooted in economics, and culture, and deeply connected to sovereignty, peace and justice. Our fight for bodily autonomy is also our fight against militarism, imperialism, and the patriarchal systems that entrench and sustain inequality. For bodily autonomy to be fully exercised, we must dismantle the pervasive systems and structures that restricts our rights. “Our fight for Sexual and Reproductive Health, Rights, and Justice is inseparable from the global struggle for justice and liberation. IPPF will always stand in solidarity with women, LGBTQI+ people, healthcare providers, and human rights defenders across the region and globally. We reject the instrumentalization of human rights as a justification for war and are steadfast and unmovable in our commitment to supporting communities who fiercely defend dignity, equality, justice, and peace.” – Maria Antonieta Alcalde, IPPF Director GeneralIPPF demands the following five actions from the U.S. and Israel: An immediate end to military escalation and attacks on civilians.Restored internet access and unhindered delivery of humanitarian and medical aid, including sexual and reproductive health services.Cessation of attacks on oil refineries.Protection of healthcare workers and facilities under international law.And an end to state repression and the release of political prisoners.Our fight for bodily autonomy, freedom and safety, is our fight against militarism and imperialism in all its forms. However the anti-rights architects attack, IPPF will be there pushing for a world that diminishes military might and machismo power structures, and defends and upholds freedom, justice, equality, and care for all.
02 April 2026
On the frontline: why local organisations are the backbone of humanitarian response in Lebanon
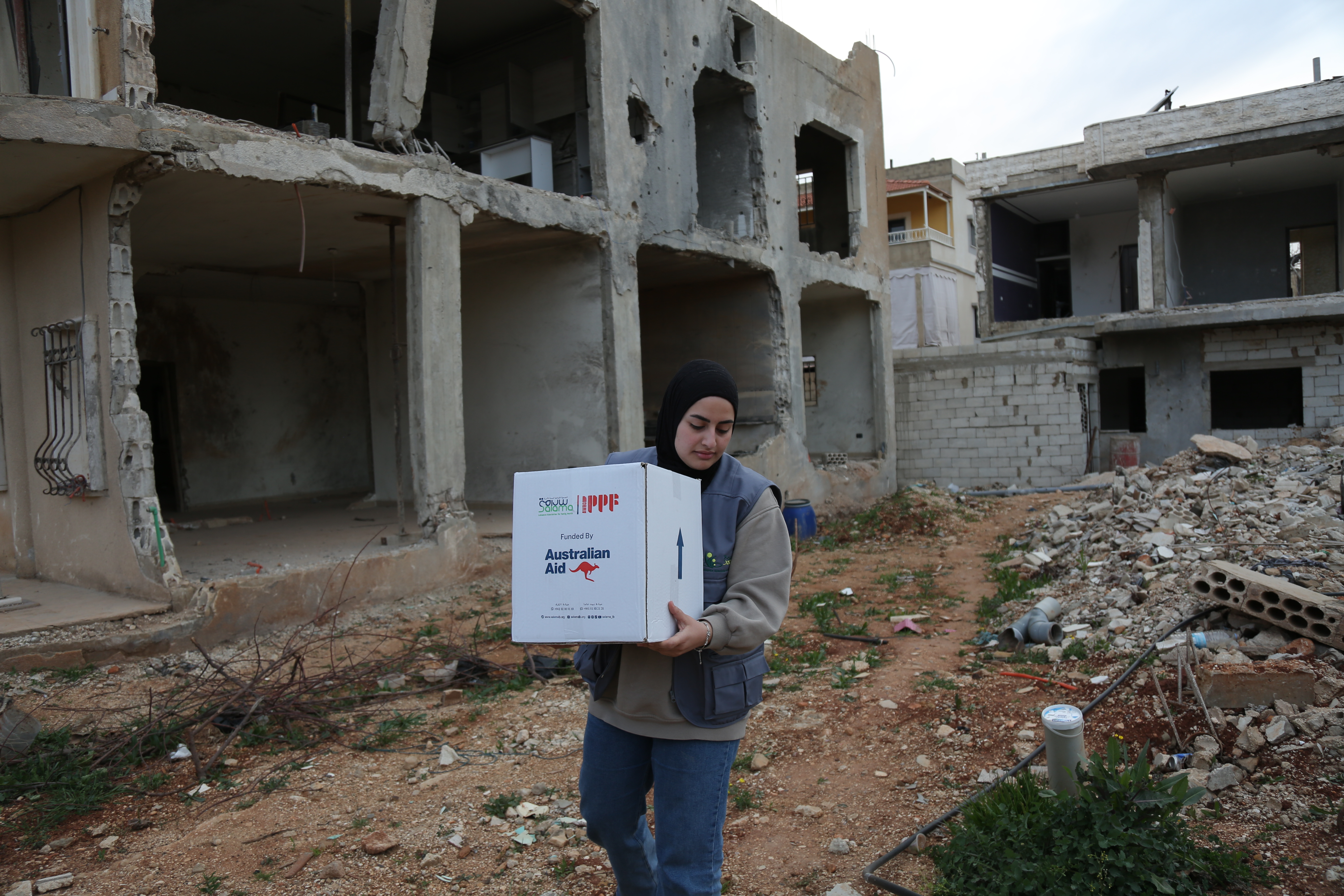
As Israeli strikes continue to drive mass displacement, casualties and destruction across Lebanon, SALAMA’s Executive Director Lina Sabra reflects on what it means to keep sexual and reproductive healthcare alive in a widening crisis. Since the latest war began on March 2nd , families across Lebanon have been fleeing Israeli attacks. More than one million people have now been displaced, and evacuation orders affect around 14 per cent of the country's territory. This escalation is unfolding amid the wider regional war, and there is a serious risk that Lebanon may once again bear the brunt of larger geopolitical agendas and be sidelined and overlooked. “They are using this moment as an opportunity for more attacks” says Lina Sabra, Executive Director of SALAMA, IPPF's Member Association in Lebanon. “That is how it feels to us. And it is our communities who are bearing the devastating consequences.” For women, girls and marginalised communities, the consequences are severe. Sexual and reproductive healthcare becomes harder to reach at the exact moment the need for it becomes more urgent. In the middle of bombing, pregnancy does not stop. Babies will still be born, in hospitals where they are still functioning, or elsewhere when they are not. Postnatal complications still require care to prevent maternal deaths. People still need contraception, medicines and menstrual hygiene supplies. Women and marginalised communities also face heightened risks of sexual and gender-based violence during humanitarian crises and need trusted, timely care. Yet these services are too often treated as secondary, even though they are central to women’s and girls’ health, dignity and survival. "Women, girls and young people are paying the price for this war in ways that are not always visible," says Lina. "Their health, safety and futures are being damaged." With support from IPPF and funding from the Government of Australia, SALAMA continues to respond every day on the ground in the Bekaa Valley in eastern Lebanon. Keeping services alive under fire National and local organisations, like SALAMA, are not standing outside the crisis looking in. They are living it while responding to it. "In the Bekaa, there are attacks every day," Lina says. "There are always warplanes, always strikes, always uncertainty. People are leaving their homes in the middle of the night when warnings come, or sometimes with no warning at all…My own family has spent one of the most terrifying nights in the car after fleeing. Staff have also been displaced. One day they are working, the next day they may have to leave their home, their town." Lina describes an assault that is targeting civilians indiscriminately. "The attacks are not only on homes and towns...they are attacking the displaced people and the camps,” Lina says. “They attacked people sheltering on the beach. They attacked the Lebanese University, killing two doctors and two scientists. And after the strikes, when the medical teams go to help, they attack them too.” No one can predict where the next strike will land or how far the conflict will spread, and Lina is worried about the uncertainty. “I have no clue. No one has. Nobody knows. Trump himself, he doesn't know. Humanitarian response cannot wait for clarity that may never come." As people flee the south and Beirut, the Bekaa has become one of the key destinations for displaced people, with families arriving in Zahlé, were SALAMA has a clinic, and the surrounding towns in large numbers. "Many are in schools. Others are in unfinished buildings or rented apartments, where landlords are multiplying costs four times over. In some places there is furniture and water. In others, there is almost nothing.” Of the more than one million people now displaced, as of March 26th, only 136,262 are registered across 663 official shelters. The rest are largely invisible to the formal system. "Many of the most vulnerable people are not in official shelters at all. They are in empty buildings, overcrowded apartments, with relatives, in places no one has formally registered. These are the people most likely to be missed, because most organisations focus on official sites. We try to reach both. Sometimes beneficiaries call us directly. Sometimes municipalities call us. Sometimes relatives tell us where families are staying. Last time, when I saw a building full of displaced families, I would go inside and ask who was responsible so we could organise distributions. This is how we work. We follow where people are." SALAMA is a small organisation, with eight staff and around 200 volunteers, but although one of its clinics has had to close, it has not stopped and it’s impact is huge. The clinic in Zahlé is providing direct clinical care, including consultations, family planning services and referrals for women who need specialist support. In the displacement shelters, SALAMA's teams are running awareness sessions, providing psychosocial support and connecting people to referral pathways for further care. Food vouchers are also being distributed to the families who need them most, with pregnant and breastfeeding women prioritised. For many of the women SALAMA reaches this combination of care, information and practical support is the only SRHiE care available. "Postnatal care is especially overlooked in a crisis”, Lina says, "Deliveries may not be safe. Women may lose access to family planning methods and other essential commodities. There are also wider health concerns linked to overcrowding, stress and poor living conditions." "Part of the team is working inside the clinic, while others are out in shelters and towns distributing dignity kits and mama and baby kits. We are using the supplies we already have, including remaining kits from IPPFs previous support and additional items received through UNFPA." SALAMA is also formally integrated into the wider humanitarian architecture, coordinating with UNFPA, UNHCR, the NGO platform and the Ministry of Public Health as part of the national response. "This is different from previous escalations," Lina says. "Before, we were often responding more independently. Now we are a wider ally of the humanitarian system, reporting activities and contributing to the national dashboard. That matters, because it helps make sexual and reproductive health in emergencies visible." What has driven that response, Lina says, is the commitment of the people delivering it. "What has stayed with me most is that our staff did not wait to be told what to do. They came forward and said they wanted to help. They wanted to go to the clinics. They wanted to support displaced people. Of course I worry about them, about their safety, about my family, about our volunteers. We assess the situation every day and adjust. But the commitment of the team is extraordinary." Rooted, trusted, ready SALAMA's strength lies not only in speed, but in the relationships that make that speed possible. Those relationships were built through the escalation of October 2024, which became a defining learning curve for the organisation. "What we have learned from previous responses has made a real difference," Lina says. "We are better prepared now because we have already lived through the worst-case scenarios. We know how to adapt. We know how to work in a fluid, fast-changing crisis." "Our staff and volunteers are from the communities affected, so they know the people, the places and the changing realities on the ground. We have direct relationships with beneficiaries, community leaders, municipalities, ministries and partners. They allow us to act quickly, identify gaps and solve problems in real time. We do not need to wait through layers of procedures before making decisions. I can take a decision, inform the staff on WhatsApp, and we move. As a local organisation, that gives us strengths that international organisations often do not have," Lina says. "Every dollar goes into the response. We are not spending money on international salaries, conferences or layers of administration. We use volunteers. We use existing clinics in the community. We adapt activities based on the situation. In war, nothing is static. People move again and again, often with no certainty about where they will end up or whether they can return. To support them, you have to be where they are." The question for humanitarian leaders and donors is a simple one: if organisations like SALAMA are already coordinated, already delivering and already trusted by the communities they serve, why are they still too often underfunded, and treated as implementers rather than leaders? Lina is clear about what she needs the international community to hear. "We need support that reaches communities through national organisations that are already there, already trusted and already responding," she says. "We need funding for services, for dignity, for health, for development. My message to donors is simple: fund communities through national NGOs." To governments, her message is equally clear. "Stop financing weapons and conflict. Girls' futures are being destroyed." She pauses. "We just need the war to stop."

Toxic Air, Lasting Harm: The Hidden Reproductive Cost of Bombing Iran’s Oil Infrastructure
As Israeli and US strikes on oil infrastructure blanketed Tehran in toxic smoke, IPPF is warning of serious, lasting risks to maternal and reproductive health - risks that are now spreading across the region.When oil infrastructure is bombed, fine particulates, soot, sulphur compounds and other toxic pollutants spread through the air, water and soil, creating serious health risks for entire communities. The World Health Organization has already warned that damage to petroleum facilities in Iran risks contaminating food, water and air supplies, with potentially severe consequences, particularly for vulnerable groups.Pregnant women and newborns are among those most at risk. There is no historical parallel for an attack on oil infrastructure of this magnitude in a city of over nine million people. However, a substantial body of research on air pollution and petroleum-related contamination points to the potential consequences for pregnant women.The environmental and public health threat extends well beyond Iran's borders. The head of the International Energy Agency warned this week that at least 40 energy assets across nine countries in the Middle East have sustained severe or critical damage since the outbreak of the war. Yet the reproductive health consequences remain entirely absent from public and political debate. Toxic smoke and the harms to pregnancy According to the Conflict and Environment Observatory (CEOBS), oil fires of this kind generate particulate matter, carbon monoxide, sulphur dioxide, nitrogen oxides and volatile organic compounds. Doug Weir, Director of the CEOBS, warns that:"The intensive use of explosive weapons in a densely populated area like Tehran generates a diverse mixture of pollutants, including pulverised building materials, heavy metals, particulate matter and explosives residues. When you include pollution from oil facility fires it is clear that pregnant women are being exposed to a complex mixture of pollutants during a period where stress may also contribute to increased vulnerability to harm." Four oil facilities in and around the city were struck, including the Tehran refinery, which has the capacity to process 225,000 barrels of oil per day. Tehran's geography makes this exposure particularly acute: the city sits in a semi-enclosed basin surrounded by the Alborz mountains, which trap pollutants within the city boundary rather than dispersing them. Reports have also described ‘black’ rain over Tehran, which can further contaminate water sources, soil and food supplies.These are the same substances that research consistently identifies as potentially harmful to a woman and her foetus during pregnancy. What we are yet to ascertain is the level and length of exposure women in Tehran will be subject to. What the evidence tells us: increased risk of preterm birth, low birth weight and miscarriageMaternal exposure to oil pollution is a significant public health concern, as exposure to air pollutants during critical stages of foetal development may lead to serious long-term adverse pregnancy outcomes¹. According to the Institute for Health Metrics and Evaluation, in its 2023 Global Burden of Disease study, 32% of preterm births in 2023 were attributed to exposure to PM air pollution². A systematic review published in JAMA Network Open reinforces this picture, analysing data from over 32 million births across over 50 studies. The study found that exposure to pollutants, particularly through fine particulate matter, was associated with an increased risk of preterm birth in 79% of studies and low birth weight in 86% of studies.³ A global meta-analysis published in PLOS Medicine, covering 204 countries and territories, found an 11% greater risk of low birth weight and a 12% greater risk of preterm birth for every 10 micrograms per cubic metre increase in exposure to fine particulate matter.⁴In addition to the risk associated with particulate matter, the fires generate neurotoxic compounds called polycyclic aromatic hydrocarbons (PAHs), formed during incomplete combustion. These compounds cross the placenta, resulting in reduced birthweight, smaller head circumference and longer-term cancer risk and cognitive deficits in offspring. Evidence comes from studies in New York⁵ ⁶, Krakow⁷, and the Gulf War oil fires ⁸ . According to Virginia Rauh, Professor of Population and Family Health at the Columbia University Mailman School of Public Health:“This multi-layered mixture of pollutants has an immediate adverse impact on fetal growth and longer-term consequences for newborn lungs and brain development, resulting in a devastating public health scenario for reproductive and child health.”Research specifically examining petroleum pollution, points to a wider pattern of reproductive harm. A 2025 systematic review and meta-analysis in BMC Pregnancy and Childbirth, found possible associations between maternal exposure to oil and gas processes and adverse outcomes including preterm birth and miscarriage.¹⁰ Whilst a prospective cohort study of 1,418 pregnant women in the Niger Delta, Nigeria, found that women in the most exposed communities faced significantly higher rates of premature rupture of membranes, postpartum haemorrhage and caesarean section compared to women in low-exposure areas.¹¹ A health crisis that could last generationsThe research points to a warning that IPPF's Global Humanitarian Director, Valerie Dourdin, says we cannot afford to ignore.“What may be framed politically as a short-term war will not produce only short-term consequences. The effects of destroying oil infrastructure do not end when the fires are extinguished. Contamination lingers in the air, in the water, in soil, and in people’s bodies. The full scale of what is unfolding over Tehran cannot yet be measured. The respiratory hazard is severe, but the evidence gives us real cause to believe this could also become a reproductive health emergency, with devastating consequences for the Iranian people, particularly women and families.”These health risks do not exist in isolation. They are compounded by the conditions of conflict itself. Women and girls in Iran already faced significant barriers to reproductive healthcare, and emergencies deepen those barriers further. In emergencies, sexual and reproductive health is routinely deprioritised. Antenatal and postnatal care is often disrupted or made unavailable. Contraception becomes harder to access, increasing unintended pregnancy and associated risks during pregnancy. Referral pathways for obstetric emergencies break down. Health workers are displaced or unable to reach those who need them, and clear public health guidance on exposure risks may be absent or inaccessible. IPPF calls on all parties, humanitarian actors and public health authorities to act with urgency. Sexual and reproductive health must be recognised as essential from the very outset of any emergency response. This means: Ensuring continuity of maternal and newborn care, including antenatal and postnatal care and emergency obstetric services.Continued and sustained active monitoring of air, water and soil contamination in Tehran must be treated as integral to protecting women's health.Increased public health measures such as awareness and clear guidance to reduce exposure risks to toxic fumes, polluted water bodies and contaminated food for pregnant people and newborns.Continuation of referral pathways and care for survivors of sexual violence and intimate partner violence.Ensuring STI and HIV screening, diagnosis and treatment services are available.Ensuring that women and girls affected by crises can access accurate SRH information, and the resources needed to manage menstruation safely and with dignity.Women's health, dignity and rights must not become collateral damage in the attacks on Iran. The evidence is worrying. Air pollution and petroleum-related contamination can harm pregnancy outcomes and threaten longer-term reproductive health. The political framing of this conflict as short-term does not change what the science tells us about the physical and psychological consequences that may follow. References¹ The associations between air pollution and adverse pregnancy outcomes in China. Tan Y, Yang R, Zhao J, Cao Z, Chen Y, Zhang B. Adv Exp Med Biol. 2017;1017:181–214. doi: 10.1007/978-981-10-5657-4_8.|² https://www.healthdata.org/research-analysis/health-topics/air-pollution³ Bekkar B et al (2020) Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US: a systematic review: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2767260⁴ Ghosh R et al. (2021) Ambient and household PM2.5 pollution and adverse perinatal outcomes: A meta-analysis and estimates of population attributable fractions globally, regionally and nationally. https://pmc.ncbi.nlm.nih.gov/articles/PMC8478226/⁵ Prenatal exposure to air pollution during the early and middle stages of pregnancy is associated with adverse neurodevelopmental outcomes at ages 1 to 3 years. Perera F, Miao Y, Ross Z, Rauh V, Margolis A, Hoepner L, Riley KW, Herbstman J, Wang S. Environ Health. 2024 Oct 30;23(1):95. doi: 10.1186/s12940-024-01132-9.PMID: 39478594 .⁶ Prenatal exposure to air pollution is associated with altered brain structure, function, and metabolism in childhood. Peterson BS, Bansal R, Sawardekar S, Nati C, Elgabalawy ER, Hoepner LA, Garcia W, Hao X, Margolis A, Perera F, Rauh V.J Child Psychol Psychiatry. 2022 Nov;63(11):1316-1331. doi: 10.1111/jcpp.13578. Epub 2022 Feb 14.PMID: 3516589⁷ Prenatal ambient air exposure to polycyclic aromatic hydrocarbons and the occurrence of respiratory symptoms over the first year of life. Jedrychowski W, Galas A, Pac A, Flak E, Camman D, Rauh V, Perera F.Eur J Epidemiol. 2005;20(9):775-82. doi: 10.1007/s10654-005-1048-1.PMID: 16170661⁸ 1991 Gulf War exposures and adverse birth outcomes. Arnetz B, Drutchas A, Sokol R, Kruger M, Jamil H.US Army Med Dep J. 2013 Apr-Jun:58-65.PMID: 23584910 ⁹Latifi Z et al. (2025) Association between maternal exposure to oil and gas extraction process with adverse birth outcomes: a systematic review and meta-analysis. BMC Pregnancy and Childbirth. https://link.springer.com/article/10.1186/s12884-025-08022-z¹⁰Oghenetega OB et al. (2022) Exposure to oil pollution and maternal outcomes: The Niger Delta prospective cohort study. _https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0263495

05 March 2026
“We need each other more than ever. We have to lift each other up.”
In the West Bank, persistent attacks, roadblocks, and an oppressive Israeli military presence are cutting women and girls off from life-saving sexual and reproductive healthcare. But, for International Women’s Day, we've collaborated with Palestinian photographer Samar Hazboun, to celebrate the determined Palestinian female doctors, social workers, health workers and communities going the extra mile for vital care.On the southern edge of a village tucked deep into the hills in the West Bank, stands a single white caravan. This modest structure is where Hiba, 26, lives with her husband and three young daughters. Under the hot sun, and with her children in tow, pregnant Hiba (pictured below) makes her way to a mobile clinic that has arrived nearby.Inside, Palestinian Family Planning and Protection Association (PFPPA) staff welcomed mothers like Hiba for a day of free sexual and reproductive health services. Their vital work is designed to reach women in precisely these areas of the West Bank - isolated, targeted and overlooked. Hiba has experienced multiple miscarriages, a reality that weighs heavily on her as she seeks care. “I came today not just to check on my pregnancy,” Hiba said, “but to show that we need more doctors and health services to meet us halfway when we can’t get to them.”The devastating destruction of health facilities by Israeli forces, severe restrictions on movement, and raids and attacks on communities in the West Bank mean Palestinians are facing increasing challenges and risks when it comes to seeking health care. In May 2025, UNFPA estimated 14,800 pregnant women in the West Bank faced limited or no care, and over 1,600 births were expected to take place in unsafe conditions. Nearly 1,000 Israeli checkpoints, gates, and roadblocks have made access to essential services nearly impossible.“The army barely allows us to breathe”, says Haneen, (pictured below right) a mother of three who has walked for two hours to reach a clinic.Hiba knows all too well that these barriers don’t just cost time, they cost lives: “A few months ago, I lost my baby son at four months old…He was the boy I always prayed for,” she said. “But we had no clinic here, and no way to get to one in time. I waited for hours for a ride. He didn’t make it.” In the face of escalating conflict and ever-tightening restrictions on movement, in 2024 PFPPA took their life-saving services to those women cut off from care. Travelling to some of the most hard-to-reach areas, their mobile clinics contain laboratory equipment, ultrasound devices and medication which would otherwise be inaccessible or unaffordable for most of the women in these communities.“Reaching remote villages is never easy - blocked roads, settler threats, or sudden orders to turn back are constant, but we try,” said Dr. Ghada, (pictured above left) a gynaecologist and obstetrician for 15 years. “Every woman deserves care.” Shayma, 22, visited a mobile clinic for a check up as her two children waited nearby:“We’re under serious economic pressure since this war started. Unemployment is up, and movement restrictions make everything harder.” Alongside maternity care, the clinics also provide wider sexual and reproductive health care, including care and advice around contraception and support related to gender-based violence. Kifah, (pictured below) 37, mother of six and an Islamic Studies graduate, knows that knowledge is power - even in crisis.“I’ve been putting myself last,” she said, describing months of delays in seeking gynaecological care. Checkpoints, settler threats, and fear have kept her confined. “Family planning is part of self-care. It’s a right, and it’s responsible, especially now.” She shares this message with other women in her village, telling them that caring for themselves and their reproductive health is an act of strength.Aya, 23, is a mother of two who remembers a neighbour forced to give birth at a checkpoint. She hopes to get an IUD to avoid an unintended pregnancy. “I can’t bring another child into this and tell them I can’t even afford a toy,” she said. So far, these mobile clinics have provided over 60,000 medical services to more than 10,000 people that may otherwise have received no sexual and reproductive healthcare. As well as the clinics, with funding from the Japan Supplementary Budget (JSB), PFPPA have also run ‘preparing for birth’ sessions, midwifery home visits, and community-based awareness sessions around safe childbirth and reproductive health. Maysa Shalaldeh (pictured above left) is an experienced psycho-social worker and the Gender Focal Person in PFPPA, delivering gender-based violence related services for women. Born and raised in Hebron, she is clear about the layered challenges Palestinian women face: legal discrimination, social stigma, economic pressure, and military occupation:“We can’t talk about rights with someone who’s struggling to afford food,” she says. “We meet people where they are. In some places, we start with nutrition or hygiene. In others, we talk about safety or mobility. Then, when there’s trust, we talk about family planning or empowerment. They are survivors. They are women with strength and dignity, navigating unimaginable hardship.”Determined, courageous women like Maysa are the cornerstone of PFPPA’s work - from social workers and pharmacists to doctors and health workers. A nurse with nearly 20 years of experience, Lubna (pictured above right) works at the mobile clinics, helping women feel safe and heard, and guiding them through their options:“I keep learning about reproductive health because I want to empower others. We live in a society where women always put themselves last. I try to show them: we put you first, because you matter.” Shaima, 27, a pharmacist with PFPPA, lights up when talking about her work. “This is the most meaningful part of my job - reaching women we’d never reach otherwise,” she said. In remote villages, she distributes medication and offers advice, but also something less tangible: trust. “I feel proud every time a woman asks me a question she was afraid to ask before,” she says. “They need more than medicine - they need someone who listens.” The work of these women has inspired others to learn and share their knowledge within their communities. Aida, (pictured above) is a mother of six and a community leader. After joining training sessions with PFPPA in reproductive health, she now volunteers with her local women’s association to share her knowledge:“We need each other more than ever. These pressures keep us from making the decisions we need. We have to lift each other up.” For women like Hiba, still reeling from the loss of her young baby, and facing the terrifying prospect of giving birth again without medical care, PFPPA’s support is a lifeline. And, along with the hundreds of women who walk through the doors of their mobile clinics, she demands a safer future for herself and her family:“I have to believe there’s a better world waiting. For my girls. For this baby. Freedom is not worrying about checkpoints. It’s giving birth safely. It’s walking to a clinic without fear. Family planning is wise. It’s power. We women need to be heard. We know what’s best for our bodies and our families.”Her words echo the determination of thousands of Palestinian women - patients, doctors, midwives, psychologists, and volunteers - who continue to protect one another’s health and dignity despite the barriers around them. Their work is not only care - it is resistance, resilience, and hope. This work was made possible thanks to generous funding from the Government of Japan.

SALAMA Concludes Japan-Funded Project to Strengthen Maternal and Reproductive Health for Vulnerable Communities in Lebanon
Beirut, Lebanon - The Lebanese Association for Family Health (SALAMA)—IPPF’s Member Association in Lebanon—hosted the closing ceremony of its Japan-funded project, “Preventing Maternal and Reproductive Health Morbidities and Mortalities among Crisis-Affected Populations, IDPs, Syrian Refugees, and Host Communities in Lebanon,” in Beirut, in the presence of a panel of participants, including the representatives of the Lebanese Ministries of Health and Social Affairs, the Government of Japan, and the IPPF.Funded through the Japan Supplementary Budget (JSB) 2024, the initiative has significantly enhanced access to lifesaving maternal and sexual and reproductive health (SRH) services for crisis-affected communities in Lebanon’s Bekaa Valley, including internally displaced persons (IDPs), Syrian refugees, and host communities.Project Achievements:85,684 SRH services delivered, reaching 28,562 beneficiaries.5,836 women received comprehensive maternal, newborn, and child health care.134 safe deliveries supported through partner hospitals.Sustained operation of two SALAMA clinics in the Bekaa Valley.Community outreach reached 5,960 individuals, with 200 mama-baby kits and 3,000 dignity kits distributed.Capacity-building trainings strengthened healthcare providers’ skills, while partnerships with municipalities and humanitarian actors ensured wider outreach and sustainability.Since 2017, Lebanon has faced overlapping crises—including economic collapse, the Beirut Port explosion, and regional conflicts—that have placed immense strain on its healthcare system. Vulnerable populations, particularly women, girls, IDPs, and refugees, have been disproportionately affected.With the generous support of the Government of Japan, SALAMA has implemented three humanitarian projects funded through the Japan Trust Fund (JTF) and JSB, delivering over 196,441 SRH services in the Bekaa Valley. These interventions have strengthened community resilience, ensured continuity of lifesaving services during prolonged crises, and integrated SRH, mental health, and gender-based violence (GBV) services through structured referral mechanisms. “The completion of this vital project in the Bekaa Valley exemplifies Japan’s steadfast commitment to protecting Sexual and Reproductive Health and Rights,” said Japan’s Ambassador to Lebanon, H.E. Kenji Yokota. “Beyond the provision of essential medical services, it upholds the fundamental right of every individual to live with dignity. This initiative embodies our Human Security approach by empowering individuals and ensuring that no one is left behind,” he added. “Japan remains dedicated to standing alongside Lebanon in supporting resilience, recovery, and long-term stability," he stressed.“From our very first steps, the Government and people of Japan have stood beside SALAMA, enabling us to serve and empower communities through years of crisis,” said Lina Sabra, Executive Director of SALAMA. “Their support, particularly in this recent project, has been a lifeline for families rebuilding after conflict. We are deeply grateful for this enduring partnership.”Through these initiatives, SALAMA has reinforced human security by protecting vulnerable individuals from disease, violence, and psychological distress, while empowering them to make informed decisions about their health and strengthening solidarity within families, communities, and health systems.About SALAMAThe Lebanese Association for Family Health “SALAMA” was founded in 2008. It is a member association of the International Planned Parenthood Federation (IPPF) which is the largest voluntary non-governmental organization in the world, working on sexual and reproductive health and rights (SRHR) issues and advocating for them. SALAMA promotes and provides high quality services, and raises awareness for all groups in the society, particularly the under-served and marginalized.About IPPFThe International Planned Parenthood Federation (IPPF) is a global federation of more than 100 locally led Member Associations working in over 150 countries to advance sexual and reproductive health and rights. In humanitarian settings, IPPF plays a critical role in delivering lifesaving maternal, sexual and reproductive health services to crisis-affected communities, including displaced populations and those facing conflict, disaster, and instability. Through its locally rooted Member Associations, IPPF provides frontline health care, supports preparedness and emergency response, strengthens health systems, and advocates for the protection of rights and dignity in even the most challenging contexts. Locally led and globally connected, IPPF combines service delivery, policy advocacy, and community engagement to ensure that no one is left behind, particularly those most underserved in humanitarian crises.

10 December 2025
Connecting Survivors to Care: A Multi-Layered Sexual and Gender-Based Violence Humanitarian Response in Sudan
The last two years of war between the Sudanese Armed Force and Rapid Support Forces have displaced over 10 million people in Khartoum, the nation’s capital, alongside regions like Darfur and Al Jazirah state. Half of the population is estimated to face acute food insecurity and there have been over 600 attacks on healthcare personnel since April 15 2023, with four attacks on healthcare facilities in January 2025. While recent statistics on maternal and reproductive health have been largely unavailable due to the conflict, maternal mortality in Sudan was among the highest in the world prior to April 2023 and access to quality sexual and reproductive healthcare has been impeded by displacement-related loss of healthcare personnel. Access to SRH services has been further impeded by stockouts of essential medicines such as emergency contraception, injectable long-acting contraception, and antibiotics for sexually transmitted infections.Despite widespread underreporting of SGBV due to cultural stigma, there are indications that sexual violence has been weaponized as an act of war. In Al Jazirah state, government officials have reported 890 cases of rape perpetrated by RSF members, resulting in 125 unwanted pregnancies. In some cases, sexual violence has resulted in severe injury and death. Women have reported both suicidal ideation and attempt after experiencing sexual violence. The actual numbers are expected to be much higher than what was recorded. Indeed, most cases and stories have gone untold; women’s rights activists estimate that only 2% of cases are reported in Sudan, and globally only 1% of adolescent girls seek help after experiencing sexual violence.In addition to risks of sexual violence as a weapon of war by armed groups, internally displaced women face sexual exploitation within temporary resettlement and camp sites. School buildings and other facilities have been repurposed to house displaced families and there are often over ten people residing together from multiple families within the same room. In this context, there is no privacy, and these risks to women are compounded within host communities, where women often receive threats as they leave IDP sites to look for work or to purchase needed resources for their families.In this context of amplified risks of SGBV and unmet need for healthcare services, the Sudanese Family Planning Association has worked with partner organizations to provide comprehensive care to SGBV survivors and has utilized social media to raise awareness about SGBV and available services for survivors. SFPA operates a four-pronged approach to addressing SGBV. Through a combination of direct clinical service points, partnerships and coordination with other NGOs, group-based discussions and individual home visits, SRH hotline, and social media strategy, the organization has been connecting survivors to care, providing medical services and referrals, and raising awareness and challenging stigmatization of SGBV.SFPA operates 26 static clinics and has used multiple mechanisms to provide services across the development-humanitarian nexus. Through 39 mobile service delivery team deployments to reach IDP camps, SFPA reached over 20,000 people displaced by conflict in Umrakoba & Tunaydbah between June and November 2024. In addition to directly providing clinical SRH and SGBV services, mobile service delivery teams shared information about SGBV to 4,506 individuals through a combination of 1499 group-level awareness raising sessions in clinic waiting areas and home visits to assess health needs on a more confidential basis. Female youth attending group-based sessions in Umrakoba & Tunaydbah shared that they gained awareness about their rights and referral pathways for violence, and adult women reported that they learned strategies for protecting and listening to their children. At these first points of in-person contact, staff have received a number of SGBV disclosures and referred survivors to clinical services.In addition to clinical services and in-person awareness-raising activities, SFPA has supported comprehensive care through coordination and partnerships with local and international NGOs. Survivors of sexual and gender-based violence must navigate a complex legal terrain as abortion is a crime in Sudan, only legally permissible in cases of rape, threats to the pregnant woman’s life, and foetal death within the womb. Women who become pregnant due to rape need police permission to undergo an abortion. In cases of pregnancy due to rape, partner organization Mutawinat obtains permission from police offices to provide abortion and SFPA directly performs the abortion for clients. SFPA also partners with an organization which provides shelter for women who become pregnant to ensure shelter and care through birth, and another organization provides financial support after birth. SFPA has also expanded access to care through implementation of a call center, or hotline, for SGBV. The call center directly serves survivors through a hotline which connects them to an integrated care team comprised of an obstetrician, family planning providers, and psychosocial support counsellors. By calling a central number – 1700 – survivors can share information about their needs and connect to available services. In 2024, the hotline received a total of 79,900 calls and provided 1,544,297 digital services. SFPA provided 2,331 SGBV services, and 60% of digitally referred SGBV cases were followed up through health service delivery points. As the war intensified and over 50% of healthcare facilities closed in conflict-affected areas, the hotline became a lifeline for accessing health care, and 45.1% (696,186) of digital services were provided for non-SRH issues.These services are complemented by a social media-based SGBV awareness strategy, implemented by youth workers connected to each SFPA branch. Through social media outlets such as TikTok, Facebook, and WhatsApp, SFPA has reached over 500,000 community members with information on SRHR and SGBV and challenging stigmatization of survivors. Youth workers have created virtual contests and games which have resulted in increasing engagement over time, with 37,000 interactions via Facebook alone.SFPA’s social media strategy has yielded a surprising result: survivors have directly responded to campaigns implemented through outlets to seek resources for support. Social media posts have shared information about SFPA’s hotline and comms staff have provided referrals to clinical services. The organization identified 5,193 clients seeking SRH services through social media outreach, including for SGBV. SFPA’s Dr Limiaa Khalfalla noted the importance of handling such disclosures carefully and ensuring adequate training to protect confidentiality. The call center has been an essential service in responding to these disclosures as a central point of referral where survivors can readily access trained staff. Through IPPF’s STREAM3 funding, SFPA has trained ten employees and eighteen volunteers on topics such as SGBV fundamentals, the LIVES approach, clinical management of rape, and long-acting contraceptive methods.

09 December 2025
Under Siege and Out of Reach: Health, Safety, and Dignity in Sudan
For more than 18 months, el-Fasher has been under siege. Families who once fled to this city in North Darfur for safety are now trapped in it. Around 260,000 civilians – including 130,000 children – are trapped with almost no aid. Food prices have soared, water is unsafe, and bombardment is constant. Those who manage to escape towards Tawila face attacks and extortion on the road. For women and girls, every stage of this journey, staying, fleeing, or arriving in displacement sites, comes with overwhelming, life-threatening risks. Across Sudan, the war between the Sudanese Armed Forces and the Rapid Support Forces (RSF) has driven one of the world’s fastest-growing displacement and hunger crises. Starvation is being used as a tactic of war, with el-Fasher a stark example. The scale of atrocities have drawn the attention of UN genocide prevention experts, and all the while, devastation spreads like wildfire. Within this wider collapse, the sexual and reproductive health and rights (SRHR) of women and girls are being systematically eroded. Gendered violence and SRHR under siegeWomen and girls in el-Fasher describe life under siege as “death by missiles, starvation and daily violations”. Families are surviving on animal feed and leaves. Girls often eat last and least, if at all. Malnutrition is rising sharply among pregnant women, new mothers and young children, heightening risks of maternal death, unsafe childbirth, and child and infant deaths. Conflict-related sexual violence has surged. Reports from el-Fasher and surrounding areas point to horrific crimes of abduction for ransom, sexual assault, and captivity as civilians attempt to move in or out of the city. Young people are particularly exposed, both during flight and in overcrowded camps where lighting, privacy and safe WASH facilities are scarce. Access to post-rape care – including emergency contraception, HIV prophylaxis, safe abortion, and psychosocial support – is extremely limited. The health system that should protect women’s lives has itself become a target. In October, armed men attacked Saudi Maternity Hospital, the only partially functioning hospital left in el-Fasher at the time. More than 460 patients and their companions were reportedly killed, and six health workers abducted, in what the World Health Organization has condemned as a flagrant attack on health care. Many of those killed and injured were women in labour and newborns. This is not an isolated incident. Clinics have been looted or destroyed, staff have fled or been killed, and basic supplies, from blood bags to oxytocin, have run out. The result is that women are giving birth at home, on the road, or in makeshift shelters without skilled care. Complications that should be easily managed are becoming fatal. At the same time, contraceptive stocks are depleted, increasing the risk of unintended pregnancies in a context of extreme violence and hunger. UN Women, UNFPA, WHO and others have documented how these patterns are not accidental but part of a broader assault on women’s rights and bodily autonomy in Sudan. Together they amount to a major rollback of SRHR gains achieved over decades, and a direct attack on the core of the Women, Peace and Security agenda. The WPS agenda recognises that women are disproportionately affected by conflict and must be given space to actively participate, be heard and represented in all peace and security processes. You can read more in UN Women’s explainer on the WPS agenda and in our factsheet on why SRHR must be part of WPS. Women are being targeted – and often the first to respondWhile formal systems collapse, Sudanese women’s organisations and health workers are holding the line. Local groups in conflict-ridden contexts have set up communal kitchens, organised food sharing, and identified malnourished children and pregnant women most in need of support. They provide information on contraception, support survivors of violence, and coordinate safe spaces in displacement camps. These are not external actors parachuting in; they are women from affected communities, doing protection and relief work often without pay or protection. Sexual and reproductive health services are still being provided in some areas by midwives, nurses and doctors working with Sudanese organisations, UN agencies and international NGOs. UNFPA and partners have supported emergency obstetric and newborn care in sites like Tawila, where many of those fleeing el-Fasher arrive. But insecurity and funding gaps mean these services reach only a fraction of those who need them. The Sudan Family Planning Association (SFPA), member association of IPPF in Sudan, has been at the forefront of this work. End of October, SFPA reported that one staff member has been detained and nine others remain missing after targeted attacks in el-Fasher; several of its clinics have been destroyed. SFPA had helped to improve Saudi Maternity Hospital’s capacities prior to the October massacre. Despite the loss of colleagues, facilities and equipment, SFPA and IPPF continue to provide SRHR services where they can – often through mobile teams and community networks – and to call for protection of health workers and facilities. This is the Women, Peace and Security (WPS) agenda in practice: women not only experiencing the worst impacts of conflict, but also at the front of humanitarian response, sustaining communities and demanding accountability. Yet they remain largely excluded from formal decision-making on ceasefires, humanitarian access and the future of Sudan. What Europe and the wider international community must doThe situation in el-Fasher is not only a humanitarian emergency; it is a test of whether governments will uphold their commitments on SRHR, international humanitarian law, and the WPS agenda during political strife. We are calling for urgent, concrete steps: Put SRHR at the centre of the humanitarian response. The EU and European governments should increase flexible humanitarian funding for Sudan, explicitly earmarking support for SRHR: emergency obstetric and newborn care, contraception, safe abortion care, and comprehensive clinical and psychosocial services for survivors of sexual violence. Funding must reach frontline providers – including SFPA, women-led organisations and community health workers.Protect women, girls and health workers. All parties to the conflict must immediately cease attacks on civilians, health facilities and humanitarian workers, in line with international humanitarian and human rights law. European governments should press for international investigations into attacks such as the Saudi Maternity Hospital massacre, and support mechanisms to document, prosecute and sanction those responsible for conflict-related sexual violence and attacks on health care. Open safe, monitored humanitarian corridors. The EU and Member States should use diplomatic and political leverage – including within the UN Security Council and regional forums – to secure a sustained ceasefire around el-Fasher and other besieged areas, and guarantee safe, unimpeded humanitarian access by land. Any “humanitarian corridor” must be genuinely safe, including for women, girls and other at-risk groups, and monitored by neutral actors.Back women’s leadership and participation. Women’s rights organisations, including those working on SRHR, must be funded and recognised as essential humanitarian and peacebuilding actors, not as add-ons. European support should enable Sudanese women peacebuilders, health workers and activists to participate meaningfully in ceasefire talks, political negotiations and reconstruction planning, in line with the WPS agenda.Sustain long-term SRHR and gender equality funding. Beyond immediate relief, the EU and European governments should protect and expand development and SRHR funding for Sudan and the region, avoiding cuts or reallocation that would further weaken fragile health systems. Investments should support comprehensive SRHR services, maternal and newborn health, adolescent girls’ health and education, and community-based work to prevent and respond to gender-based violence, including harmful practices such as FGM. The war in Sudan, the siege of el-Fasher in particular, is exposing just how quickly women’s and girls’ rights can be dismantled when conflict, impunity and neglect converge. It is also showing, once again, that women are central to any meaningful response. In this devastating situation, we are calling on European countries and the European Union to take urgent action to uphold the rights, health, and dignity of Sudanese people. This article was originally published on countdown2030Europe.

IPPF stands against Trumps enforced silence on World AIDS Day
This year, the Trump administration has banned federal employees and grant recipients from acknowledging World AIDS Day, celebrated on the 1st December 2025. The State Department’s directive told employees to “refrain from publicly promoting World AIDS Day through any communication channels, including social media, media engagements, speeches or other public-facing messaging”.This latest directive comes after US funding cuts this year put essential sexual and reproductive healthcare, which includes HIV prevention services, at risk for millions worldwide. A global survey of Member Associations conducted by IPPF revealed the devastating impacts on our Member Associations who provide integrated sexual and reproductive healthcare services. Over half our Member Associations were affected, with an estimated loss of $85million. The Trump administration’s decision to enforce silence around World AIDS Day demonstrates a lack of respect for the lived experiences of those living with HIV, those who died of AIDS, and all affected by HIV. This directive impedes the ongoing efforts to reduce the transmission of HIV and to address stigma, discrimination, and inequality. These decisions are not isolated from broader state driven ideologies and anti-rights pushbacks that continue to suppress the acceptance and fair inclusion of all people in society. This enforced silence on World AIDS Day serves only to further embed stigma and injustice and is another reminder as to why we must confront these moments with equal strength and clarity. IPPF supports the rights of all people in society and works to provide sexual and reproductive health services to all, in particular those who are marginalised, such as gay men and other men who have sex with men, sex workers, trans people, people who inject drugs, and prisoners. IPPF works with our Member Associations doing vital work to support those living with HIV, to end stigma, and ‘overcome disruption’ to providing essential health services to communities, including HIV testing, prevention and treatment. In times of crisis and oppression, rights and dignity need champions. At IPPF we carry this moment with our Member Associations on the ground and stand behind them in their continued dignity and fight for the right to continue the vital work they do. At IPPF we will continue our work towards a vision of a world free from HIV where everyone is valued equally, has a healthy, pleasurable, and fulfilling life within a just and equal society. Key to an impactful HIV programme is understanding and addressing drivers of the HIV pandemic, including structural barriers; violence against women; discrimination; stigma; harmful social norms; inequalities related to sex, gender, sexual orientation, race, disability, and economic status; criminalisation of HIV transmission and certain populations; and restrictive laws and policies.Due to social and biological vulnerabilities, certain groups of people experience higher rates of HIV including women and girls; gay, bisexual, and other men who have sex with men; sex workers; people who inject drugs; trans people; and people in prisons. Working with those affected by and living with HIV to design, implement, and evaluate IPPF services and programmes is essential on our pathway to realise a society free of discrimination and stigma, and for all people living with HIV to live healthy and fulfilled lives. A community-led and inclusive response includes both tailoring services and programmes to address the needs of communities more severely affected by HIV, as well as addressing the needs of all people who would benefit from HIV‑related services such as youth, people with disabilities, pregnant women and infants, people in sexual relationships with individuals living with HIV, boys and men, and others who may not identify as a member of certain groups. Of key importance is creating programmes, services, and spaces that are inclusive, discrimination-free, and accessible to all, where each person feels welcomed and that their health and well‑being needs will be at the centre of the care that they receive.At IPPF our Member Association’s work demonstrates what we can achieve when we lead with community-led responses. For example, in Mozambique, the Associação Moçambicana para o Desenvolvimento da Família (AMODEFA), together with sex workers, are working to ensure that sex workers have access to comprehensive sexual and reproductive health services, with oral pre-exposure prophylaxis (PrEP*) for HIV prevention.In Zambia, the Planned Parenthood Association of Zambia (PPAZ), through a partnership between the Children’s Investment Fund Foundation (CIFF) and the Global Fund to Fight AIDS, Tuberculosis, and Malaria—has secured 21,600 Dapivirine Vaginal Rings for HIV prevention for women. Adding the PrEP ring as an additional HIV prevention option gives women more choice about which HIV prevention method they can use, empowers them to make informed decisions about their health, and increases the chance that individuals can find a method that works for them.On Worlds AIDS day we are doubling down on our commitment and support to the communities we work with and our Member Associations who continue to provide innovative healthcare models to prevent HIV transmission, and provide vital care to those living with HIV. The work in Mozambique and Zambia are just two examples of the work that many Member Associations are implementing globally to provide essential health services to communities, including HIV testing, treatment and prevention. *Pre-Exposure Prophylaxis (PrEP) is used to reduce the risk of getting HIV.
IPPF and Japan team up on another project to sustain sexual and reproductive health services in the West Bank, Palestine
21st April 2026 - IPPF and its Member Association in Palestine (PFPPA) are pleased to announce the launch of a new project financed by the Government of Japan, "Provision of health and medical services for women and children affected by crisis in the West Bank." This project will deliver life-saving maternal healthcare, psychosocial support, and sexual and reproductive health services, in even the hardest-to-reach areas of the West Bank, Palestine, through health centres, mobile medical teams, tele-consultations, and community outreach. The destruction of health facilities, severe restrictions on movement, and raids and attacks on communities in the West Bank have left Palestinians with little to no access to healthcare. According to the UNFPA, over 230,000 women and girls experience difficulties in accessing reproductive health services. Key project activities will include:Maintaining essential sexual and reproductive health (SRH) services, through three static clinics in Khalil, Halhoul and Bethlehem in the West Bank. These clinics will offer services including family planning, obstetrics and gynaecology care and management of sexually transmitted infections, for over 22,000 women and children. This will include specialised support for an estimated 2,300 survivors of sexual and gender-based violence, who will receive medical care, counselling or referrals. Providing maternal and child health care services for 4,600 women and children in hard-to-reach and marginalised areas of the West Bank via a mobile team of doctors, midwives, paediatricians, social workers, pharmacists and lab technicians. The mobile team will also provide psychosocial support services, support for survivors of sexual and gender-based violence, and family planning services. Providing counselling and consultation services via telecommunications and digital channels for those unable to access clinics.Conducting five ‘preparing for birth’ sessions for 90 first time mothers, providing information and support on maternal care and options for labour and delivery. Mr. ARAIKE Katsuhiko, Ambassador of Japan for the Palestinian Affairs says: “As a flagbearer of Universal Health Coverage (UHC) and the Women, Peace, and Security (WPS) agenda, we hope that our new collaboration with IPPF facilitates Palestinian women and children, who are affected by conflicts and live outside service catchment areas, to enjoy Obstetrics and Gynecology (OBGYN) and family planning services, improved well-being, and social participation. This project is part of Japan’s 2026–2027 cooperation package for Palestine. Japan will continue to provide support for the stability and prosperity of Palestine.” Dr. Fadoua Bakhadda, Regional Director of the IPPF Arab World Regional Office adds: “Thanks to the support of the people of Japan, we can continue delivering essential maternal and child health services to communities that have been systematically cut off from care, helping to prevent avoidable maternal and newborn deaths in the West Bank, Palestine.” -- About International Planned Parenthood Federation (IPPF) Arab World Office IPPF is a global healthcare provider and a leading advocate of sexual and reproductive health and rights (SRHR) for all. Led by a courageous and determined group of women, IPPF was founded in 1952. Today, we are a movement of over 120 autonomous member associations and 23 collaborative partners with a presence in 146 countries. Established in 1971, the IPPF Arab World Region (IPPF AWR) is one of IPPF’s six regional offices. Based in Tunis, it is the leading Sexual and Reproductive Health (SRH) service delivery organization in the North Africa and the Middle East, and the leading Sexual and Reproductive Health and Rights (SRHR) advocacy voice in the region.
Japan funds essential supplies for healthcare clinics in Sudan
16th April 2026 - A new project titled Strengthening Life-saving Sexual and Reproductive Health (SRH) Services for Internally Displaced Persons (IDPs), has been launched in Sudan. Funded by the Government of Japan and implemented by the IPPF Member Association Sudan Family Planning Association (SFPA), the project will support women and girls in crisis in the Red Sea and Khartoum States. Fifteen million people in Sudan have been displaced by the civil war, and conflicts in neighbouring countries have triggered an influx of returnees and displaced people into Sudan. As a result, the country now hosts 15% of the world’s IDPs. But widespread destruction of infrastructure and deadly disease outbreaks have left the healthcare system unable to cope.An estimated 1.75 million women and girls require urgent sexual and reproductive health (SRH) services, including 270,000 internally displaced pregnant women. With rape increasingly used as a weapon of war, many require urgent medical and psychosocial support. However, essential SRH commodities, including contraceptives, emergency obstetric kits, and menstrual hygiene products, are in critically low supply. SFPA provides essential sexual and reproductive health services to women and girls, including internally displaced persons, through 26 static clinics and 11 mobile clinics across the country. This new funding will enable them to procure, transport and distribute essential supplies to two of the organisation’s static clinics in the Red Sea State and Khartoum State. This vital equipment, including microscopes, blood-testing devices, thermometers, and examination lamps, will enable these clinics to continue providing SRH services, expanding their reach to an additional 2,400 internally displaced people and individuals in host communities. Mr. Nakahara Takanobu, the Chargé d’Affaires ad interim of the Embassy of Japan to Sudan, stated that, “The provision of sexual and reproductive healthcare for women and girls is a critical step in supporting this vulnerable category in Sudan. This is more so when they are IDPs. Thus, we are happy to be able to support IPPF’s Member Association in Sudan - the Sudan Family Planning Association - in this domain, so that we can contribute to improving the safety and well-being of these women and girls, and reassure them that we acknowledge the challenges they face and endure.” Dr Hiba Ahmed Khalil, Emergency and Humanitarian Interventions Manager at SFPA added, “SFPA is honoured to join the Japan Supplementary Budget 2025 project, advancing inclusive health and humanitarian responses that strengthen access to essential services and uphold the rights of communities most at risk. Together, we are building pathways for resilience and equity.” Dr. Fadoua Bakhadda, Regional Director of the IPPF Arab World Regional Office, added, “Every woman and girl deserves access to safe, reliable healthcare, no matter the circumstances. Thanks to the people of Japan, we can equip clinics with the essential tools and supplies needed to continue providing critical sexual and reproductive healthcare. This investment will directly improve the safety, health, and resilience of thousands of internally displaced women and girls.” ---About the Sudan Family Planning Association The Sudan Family Planning Association (SFPA) was established in 1965 by pioneers in obstetrics and gynaecology in response to increases in maternal, neonatal and infant mortality and morbidity. As the statistics show, Sudan is a country in great need of frontline sexual and reproductive health (SRH) services. Advocacy, and undertaking information, education and communication (IEC) programs are critical.About International Planned Parenthood Federation (IPPF) Arab World Office IPPF is a global healthcare provider and a leading advocate of sexual and reproductive health and rights (SRHR) for all. Led by a courageous and determined group of women, IPPF was founded in 1952. Today, we are a movement of over 120 autonomous member associations and 23 collaborative partners with a presence in 146 countries. Established in 1971, the IPPF Arab World Region (IPPF AWR) is one of IPPF’s six regional offices. Based in Tunis, it is the leading Sexual and Reproductive Health (SRH) service delivery organization in North Africa and the Middle East, and the leading Sexual and Reproductive Health and Rights (SRHR) advocacy voice in the region.
08 April 2026
IPPF Rejects the Instrumentalisation of human rights as a justification for war.
The bombing of Iran and the region by Israel and the United States is orchestrated by men who worship militarised masculinities and whose world views are founded on dominance, control, and aggression. These actions only serve their own power, and sustain systems of militarisation, imperialism and patriarchy under which women, girls, and marginalised communities disproportionality suffer. As the military assault against Iran by the US and Isreal intensifies on multiple fronts across the region, Donald Trump and Benjamin Netanyahu are using the same settler-colonial playbooks used in Gaza and further expanding it across the region. Under the pretext of “defending human rights”, Israel and the US are bombing densely populated areas and forcing entire communities to flee as a part of its strategy of colonial expansion and regional dominance.In Iran, mandatory veiling laws, criminalisation of abortion, restrictions on contraception, and the violent suppression of feminist activists is now being met with aerial bombardment. Women, girls, and marginalised communities are at the centre of a war between supremacists, where the dropping of bombs is the so-called precursor to peace and stability that takes the form of bombed clinics, decimated health systems, and burning oil infrastructure , which is blanketing Tehran in a toxic smoke that has lasting risks to maternal and reproductive health. In Lebanon, the destruction of infrastructure, road closures, and the constant threat of airstrikes are severely disrupting clinic activities and community health services. Many of those displaced are women and LGBTQI+ individuals who are pregnant, breastfeeding, or caring for newborns and young children, with nowhere safe to go. Overcrowded shelters often lack adequate sanitation, privacy, and basic supplies, undermining individuals' safety and mobility while heightening the risk of harassment, exploitation, and gender-based violence.All the while, the genocide in Gaza continues. Border crossings have been closed, movement in the West Bank has been shut down, and illegal settler and police violence continues whilst our attention is pulled to the multitude of crises at the hands of Donald Trump and Benjamin Netanyahu. The same ideological machismo that attacks bodily autonomy also glorifies war and destruction.The international community’s failure to stop the genocide in Gaza or enforce international humanitarian law, alongside the protection Israel receives from powerful allies, has emboldened this violence and enabled its expansion across the region and globally.The bombing and international interventions in Venezuela, Iran, Kurdistan-Iraq, Palestine, Nigeria, Somalia, Yemen and Syria, and now Lebanon, evidence how military power is being abused with no limits by the US. This use of force, bolstered by equally aggressive or compliant allies, is the new normal for the so called ‘President of Peace’.These are the same actors that are rolling back sexual and reproductive health, rights and justice (SRHRJ), and are simultaneously driving anti-LGBTQI+, and anti-migrant efforts in their own countries, while using the language of freedom to bomb others. This is matched by the scaffolding of white supremacy and a brand of masculinity that celebrates war and legitimises ultra conservative, traditionalist and illiberal leaders and authoritarian actors to leverage their foreign influence to weaken democratic norms and undermine regional security. All the while we draw on the language of a world order that is interpreted through a US and Global North centric lens, built by powerful states for powerful states on the coattails of patriarchy and colonialism. "The world we live in is designed by and for cisgender, straight men—a direct legacy of patriarchy. This same system creates and launches wars. Pregnant people, children, the elderly, and those living with disabilities or chronic illnesses are particularly vulnerable in these situations. Since caregiving is often an unpaid, unrecognized, and gendered task, women frequently bear the responsibility of caring for children and the elderly, often at the expense of their own health and needs. Furthermore, the mental health impact of war on women, girls, LGBTQIA+ individuals, and other marginalized communities remains an often overlooked issue." – Soudeh Rade, Executive Director, SpectrumBodily autonomy is not a separate issue – it is rooted in economics, and culture, and deeply connected to sovereignty, peace and justice. Our fight for bodily autonomy is also our fight against militarism, imperialism, and the patriarchal systems that entrench and sustain inequality. For bodily autonomy to be fully exercised, we must dismantle the pervasive systems and structures that restricts our rights. “Our fight for Sexual and Reproductive Health, Rights, and Justice is inseparable from the global struggle for justice and liberation. IPPF will always stand in solidarity with women, LGBTQI+ people, healthcare providers, and human rights defenders across the region and globally. We reject the instrumentalization of human rights as a justification for war and are steadfast and unmovable in our commitment to supporting communities who fiercely defend dignity, equality, justice, and peace.” – Maria Antonieta Alcalde, IPPF Director GeneralIPPF demands the following five actions from the U.S. and Israel: An immediate end to military escalation and attacks on civilians.Restored internet access and unhindered delivery of humanitarian and medical aid, including sexual and reproductive health services.Cessation of attacks on oil refineries.Protection of healthcare workers and facilities under international law.And an end to state repression and the release of political prisoners.Our fight for bodily autonomy, freedom and safety, is our fight against militarism and imperialism in all its forms. However the anti-rights architects attack, IPPF will be there pushing for a world that diminishes military might and machismo power structures, and defends and upholds freedom, justice, equality, and care for all.
02 April 2026
On the frontline: why local organisations are the backbone of humanitarian response in Lebanon
As Israeli strikes continue to drive mass displacement, casualties and destruction across Lebanon, SALAMA’s Executive Director Lina Sabra reflects on what it means to keep sexual and reproductive healthcare alive in a widening crisis. Since the latest war began on March 2nd , families across Lebanon have been fleeing Israeli attacks. More than one million people have now been displaced, and evacuation orders affect around 14 per cent of the country's territory. This escalation is unfolding amid the wider regional war, and there is a serious risk that Lebanon may once again bear the brunt of larger geopolitical agendas and be sidelined and overlooked. “They are using this moment as an opportunity for more attacks” says Lina Sabra, Executive Director of SALAMA, IPPF's Member Association in Lebanon. “That is how it feels to us. And it is our communities who are bearing the devastating consequences.” For women, girls and marginalised communities, the consequences are severe. Sexual and reproductive healthcare becomes harder to reach at the exact moment the need for it becomes more urgent. In the middle of bombing, pregnancy does not stop. Babies will still be born, in hospitals where they are still functioning, or elsewhere when they are not. Postnatal complications still require care to prevent maternal deaths. People still need contraception, medicines and menstrual hygiene supplies. Women and marginalised communities also face heightened risks of sexual and gender-based violence during humanitarian crises and need trusted, timely care. Yet these services are too often treated as secondary, even though they are central to women’s and girls’ health, dignity and survival. "Women, girls and young people are paying the price for this war in ways that are not always visible," says Lina. "Their health, safety and futures are being damaged." With support from IPPF and funding from the Government of Australia, SALAMA continues to respond every day on the ground in the Bekaa Valley in eastern Lebanon. Keeping services alive under fire National and local organisations, like SALAMA, are not standing outside the crisis looking in. They are living it while responding to it. "In the Bekaa, there are attacks every day," Lina says. "There are always warplanes, always strikes, always uncertainty. People are leaving their homes in the middle of the night when warnings come, or sometimes with no warning at all…My own family has spent one of the most terrifying nights in the car after fleeing. Staff have also been displaced. One day they are working, the next day they may have to leave their home, their town." Lina describes an assault that is targeting civilians indiscriminately. "The attacks are not only on homes and towns...they are attacking the displaced people and the camps,” Lina says. “They attacked people sheltering on the beach. They attacked the Lebanese University, killing two doctors and two scientists. And after the strikes, when the medical teams go to help, they attack them too.” No one can predict where the next strike will land or how far the conflict will spread, and Lina is worried about the uncertainty. “I have no clue. No one has. Nobody knows. Trump himself, he doesn't know. Humanitarian response cannot wait for clarity that may never come." As people flee the south and Beirut, the Bekaa has become one of the key destinations for displaced people, with families arriving in Zahlé, were SALAMA has a clinic, and the surrounding towns in large numbers. "Many are in schools. Others are in unfinished buildings or rented apartments, where landlords are multiplying costs four times over. In some places there is furniture and water. In others, there is almost nothing.” Of the more than one million people now displaced, as of March 26th, only 136,262 are registered across 663 official shelters. The rest are largely invisible to the formal system. "Many of the most vulnerable people are not in official shelters at all. They are in empty buildings, overcrowded apartments, with relatives, in places no one has formally registered. These are the people most likely to be missed, because most organisations focus on official sites. We try to reach both. Sometimes beneficiaries call us directly. Sometimes municipalities call us. Sometimes relatives tell us where families are staying. Last time, when I saw a building full of displaced families, I would go inside and ask who was responsible so we could organise distributions. This is how we work. We follow where people are." SALAMA is a small organisation, with eight staff and around 200 volunteers, but although one of its clinics has had to close, it has not stopped and it’s impact is huge. The clinic in Zahlé is providing direct clinical care, including consultations, family planning services and referrals for women who need specialist support. In the displacement shelters, SALAMA's teams are running awareness sessions, providing psychosocial support and connecting people to referral pathways for further care. Food vouchers are also being distributed to the families who need them most, with pregnant and breastfeeding women prioritised. For many of the women SALAMA reaches this combination of care, information and practical support is the only SRHiE care available. "Postnatal care is especially overlooked in a crisis”, Lina says, "Deliveries may not be safe. Women may lose access to family planning methods and other essential commodities. There are also wider health concerns linked to overcrowding, stress and poor living conditions." "Part of the team is working inside the clinic, while others are out in shelters and towns distributing dignity kits and mama and baby kits. We are using the supplies we already have, including remaining kits from IPPFs previous support and additional items received through UNFPA." SALAMA is also formally integrated into the wider humanitarian architecture, coordinating with UNFPA, UNHCR, the NGO platform and the Ministry of Public Health as part of the national response. "This is different from previous escalations," Lina says. "Before, we were often responding more independently. Now we are a wider ally of the humanitarian system, reporting activities and contributing to the national dashboard. That matters, because it helps make sexual and reproductive health in emergencies visible." What has driven that response, Lina says, is the commitment of the people delivering it. "What has stayed with me most is that our staff did not wait to be told what to do. They came forward and said they wanted to help. They wanted to go to the clinics. They wanted to support displaced people. Of course I worry about them, about their safety, about my family, about our volunteers. We assess the situation every day and adjust. But the commitment of the team is extraordinary." Rooted, trusted, ready SALAMA's strength lies not only in speed, but in the relationships that make that speed possible. Those relationships were built through the escalation of October 2024, which became a defining learning curve for the organisation. "What we have learned from previous responses has made a real difference," Lina says. "We are better prepared now because we have already lived through the worst-case scenarios. We know how to adapt. We know how to work in a fluid, fast-changing crisis." "Our staff and volunteers are from the communities affected, so they know the people, the places and the changing realities on the ground. We have direct relationships with beneficiaries, community leaders, municipalities, ministries and partners. They allow us to act quickly, identify gaps and solve problems in real time. We do not need to wait through layers of procedures before making decisions. I can take a decision, inform the staff on WhatsApp, and we move. As a local organisation, that gives us strengths that international organisations often do not have," Lina says. "Every dollar goes into the response. We are not spending money on international salaries, conferences or layers of administration. We use volunteers. We use existing clinics in the community. We adapt activities based on the situation. In war, nothing is static. People move again and again, often with no certainty about where they will end up or whether they can return. To support them, you have to be where they are." The question for humanitarian leaders and donors is a simple one: if organisations like SALAMA are already coordinated, already delivering and already trusted by the communities they serve, why are they still too often underfunded, and treated as implementers rather than leaders? Lina is clear about what she needs the international community to hear. "We need support that reaches communities through national organisations that are already there, already trusted and already responding," she says. "We need funding for services, for dignity, for health, for development. My message to donors is simple: fund communities through national NGOs." To governments, her message is equally clear. "Stop financing weapons and conflict. Girls' futures are being destroyed." She pauses. "We just need the war to stop."
Toxic Air, Lasting Harm: The Hidden Reproductive Cost of Bombing Iran’s Oil Infrastructure
As Israeli and US strikes on oil infrastructure blanketed Tehran in toxic smoke, IPPF is warning of serious, lasting risks to maternal and reproductive health - risks that are now spreading across the region.When oil infrastructure is bombed, fine particulates, soot, sulphur compounds and other toxic pollutants spread through the air, water and soil, creating serious health risks for entire communities. The World Health Organization has already warned that damage to petroleum facilities in Iran risks contaminating food, water and air supplies, with potentially severe consequences, particularly for vulnerable groups.Pregnant women and newborns are among those most at risk. There is no historical parallel for an attack on oil infrastructure of this magnitude in a city of over nine million people. However, a substantial body of research on air pollution and petroleum-related contamination points to the potential consequences for pregnant women.The environmental and public health threat extends well beyond Iran's borders. The head of the International Energy Agency warned this week that at least 40 energy assets across nine countries in the Middle East have sustained severe or critical damage since the outbreak of the war. Yet the reproductive health consequences remain entirely absent from public and political debate. Toxic smoke and the harms to pregnancy According to the Conflict and Environment Observatory (CEOBS), oil fires of this kind generate particulate matter, carbon monoxide, sulphur dioxide, nitrogen oxides and volatile organic compounds. Doug Weir, Director of the CEOBS, warns that:"The intensive use of explosive weapons in a densely populated area like Tehran generates a diverse mixture of pollutants, including pulverised building materials, heavy metals, particulate matter and explosives residues. When you include pollution from oil facility fires it is clear that pregnant women are being exposed to a complex mixture of pollutants during a period where stress may also contribute to increased vulnerability to harm." Four oil facilities in and around the city were struck, including the Tehran refinery, which has the capacity to process 225,000 barrels of oil per day. Tehran's geography makes this exposure particularly acute: the city sits in a semi-enclosed basin surrounded by the Alborz mountains, which trap pollutants within the city boundary rather than dispersing them. Reports have also described ‘black’ rain over Tehran, which can further contaminate water sources, soil and food supplies.These are the same substances that research consistently identifies as potentially harmful to a woman and her foetus during pregnancy. What we are yet to ascertain is the level and length of exposure women in Tehran will be subject to. What the evidence tells us: increased risk of preterm birth, low birth weight and miscarriageMaternal exposure to oil pollution is a significant public health concern, as exposure to air pollutants during critical stages of foetal development may lead to serious long-term adverse pregnancy outcomes¹. According to the Institute for Health Metrics and Evaluation, in its 2023 Global Burden of Disease study, 32% of preterm births in 2023 were attributed to exposure to PM air pollution². A systematic review published in JAMA Network Open reinforces this picture, analysing data from over 32 million births across over 50 studies. The study found that exposure to pollutants, particularly through fine particulate matter, was associated with an increased risk of preterm birth in 79% of studies and low birth weight in 86% of studies.³ A global meta-analysis published in PLOS Medicine, covering 204 countries and territories, found an 11% greater risk of low birth weight and a 12% greater risk of preterm birth for every 10 micrograms per cubic metre increase in exposure to fine particulate matter.⁴In addition to the risk associated with particulate matter, the fires generate neurotoxic compounds called polycyclic aromatic hydrocarbons (PAHs), formed during incomplete combustion. These compounds cross the placenta, resulting in reduced birthweight, smaller head circumference and longer-term cancer risk and cognitive deficits in offspring. Evidence comes from studies in New York⁵ ⁶, Krakow⁷, and the Gulf War oil fires ⁸ . According to Virginia Rauh, Professor of Population and Family Health at the Columbia University Mailman School of Public Health:“This multi-layered mixture of pollutants has an immediate adverse impact on fetal growth and longer-term consequences for newborn lungs and brain development, resulting in a devastating public health scenario for reproductive and child health.”Research specifically examining petroleum pollution, points to a wider pattern of reproductive harm. A 2025 systematic review and meta-analysis in BMC Pregnancy and Childbirth, found possible associations between maternal exposure to oil and gas processes and adverse outcomes including preterm birth and miscarriage.¹⁰ Whilst a prospective cohort study of 1,418 pregnant women in the Niger Delta, Nigeria, found that women in the most exposed communities faced significantly higher rates of premature rupture of membranes, postpartum haemorrhage and caesarean section compared to women in low-exposure areas.¹¹ A health crisis that could last generationsThe research points to a warning that IPPF's Global Humanitarian Director, Valerie Dourdin, says we cannot afford to ignore.“What may be framed politically as a short-term war will not produce only short-term consequences. The effects of destroying oil infrastructure do not end when the fires are extinguished. Contamination lingers in the air, in the water, in soil, and in people’s bodies. The full scale of what is unfolding over Tehran cannot yet be measured. The respiratory hazard is severe, but the evidence gives us real cause to believe this could also become a reproductive health emergency, with devastating consequences for the Iranian people, particularly women and families.”These health risks do not exist in isolation. They are compounded by the conditions of conflict itself. Women and girls in Iran already faced significant barriers to reproductive healthcare, and emergencies deepen those barriers further. In emergencies, sexual and reproductive health is routinely deprioritised. Antenatal and postnatal care is often disrupted or made unavailable. Contraception becomes harder to access, increasing unintended pregnancy and associated risks during pregnancy. Referral pathways for obstetric emergencies break down. Health workers are displaced or unable to reach those who need them, and clear public health guidance on exposure risks may be absent or inaccessible. IPPF calls on all parties, humanitarian actors and public health authorities to act with urgency. Sexual and reproductive health must be recognised as essential from the very outset of any emergency response. This means: Ensuring continuity of maternal and newborn care, including antenatal and postnatal care and emergency obstetric services.Continued and sustained active monitoring of air, water and soil contamination in Tehran must be treated as integral to protecting women's health.Increased public health measures such as awareness and clear guidance to reduce exposure risks to toxic fumes, polluted water bodies and contaminated food for pregnant people and newborns.Continuation of referral pathways and care for survivors of sexual violence and intimate partner violence.Ensuring STI and HIV screening, diagnosis and treatment services are available.Ensuring that women and girls affected by crises can access accurate SRH information, and the resources needed to manage menstruation safely and with dignity.Women's health, dignity and rights must not become collateral damage in the attacks on Iran. The evidence is worrying. Air pollution and petroleum-related contamination can harm pregnancy outcomes and threaten longer-term reproductive health. The political framing of this conflict as short-term does not change what the science tells us about the physical and psychological consequences that may follow. References¹ The associations between air pollution and adverse pregnancy outcomes in China. Tan Y, Yang R, Zhao J, Cao Z, Chen Y, Zhang B. Adv Exp Med Biol. 2017;1017:181–214. doi: 10.1007/978-981-10-5657-4_8.|² https://www.healthdata.org/research-analysis/health-topics/air-pollution³ Bekkar B et al (2020) Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US: a systematic review: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2767260⁴ Ghosh R et al. (2021) Ambient and household PM2.5 pollution and adverse perinatal outcomes: A meta-analysis and estimates of population attributable fractions globally, regionally and nationally. https://pmc.ncbi.nlm.nih.gov/articles/PMC8478226/⁵ Prenatal exposure to air pollution during the early and middle stages of pregnancy is associated with adverse neurodevelopmental outcomes at ages 1 to 3 years. Perera F, Miao Y, Ross Z, Rauh V, Margolis A, Hoepner L, Riley KW, Herbstman J, Wang S. Environ Health. 2024 Oct 30;23(1):95. doi: 10.1186/s12940-024-01132-9.PMID: 39478594 .⁶ Prenatal exposure to air pollution is associated with altered brain structure, function, and metabolism in childhood. Peterson BS, Bansal R, Sawardekar S, Nati C, Elgabalawy ER, Hoepner LA, Garcia W, Hao X, Margolis A, Perera F, Rauh V.J Child Psychol Psychiatry. 2022 Nov;63(11):1316-1331. doi: 10.1111/jcpp.13578. Epub 2022 Feb 14.PMID: 3516589⁷ Prenatal ambient air exposure to polycyclic aromatic hydrocarbons and the occurrence of respiratory symptoms over the first year of life. Jedrychowski W, Galas A, Pac A, Flak E, Camman D, Rauh V, Perera F.Eur J Epidemiol. 2005;20(9):775-82. doi: 10.1007/s10654-005-1048-1.PMID: 16170661⁸ 1991 Gulf War exposures and adverse birth outcomes. Arnetz B, Drutchas A, Sokol R, Kruger M, Jamil H.US Army Med Dep J. 2013 Apr-Jun:58-65.PMID: 23584910 ⁹Latifi Z et al. (2025) Association between maternal exposure to oil and gas extraction process with adverse birth outcomes: a systematic review and meta-analysis. BMC Pregnancy and Childbirth. https://link.springer.com/article/10.1186/s12884-025-08022-z¹⁰Oghenetega OB et al. (2022) Exposure to oil pollution and maternal outcomes: The Niger Delta prospective cohort study. _https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0263495
05 March 2026
“We need each other more than ever. We have to lift each other up.”
In the West Bank, persistent attacks, roadblocks, and an oppressive Israeli military presence are cutting women and girls off from life-saving sexual and reproductive healthcare. But, for International Women’s Day, we've collaborated with Palestinian photographer Samar Hazboun, to celebrate the determined Palestinian female doctors, social workers, health workers and communities going the extra mile for vital care.On the southern edge of a village tucked deep into the hills in the West Bank, stands a single white caravan. This modest structure is where Hiba, 26, lives with her husband and three young daughters. Under the hot sun, and with her children in tow, pregnant Hiba (pictured below) makes her way to a mobile clinic that has arrived nearby.Inside, Palestinian Family Planning and Protection Association (PFPPA) staff welcomed mothers like Hiba for a day of free sexual and reproductive health services. Their vital work is designed to reach women in precisely these areas of the West Bank - isolated, targeted and overlooked. Hiba has experienced multiple miscarriages, a reality that weighs heavily on her as she seeks care. “I came today not just to check on my pregnancy,” Hiba said, “but to show that we need more doctors and health services to meet us halfway when we can’t get to them.”The devastating destruction of health facilities by Israeli forces, severe restrictions on movement, and raids and attacks on communities in the West Bank mean Palestinians are facing increasing challenges and risks when it comes to seeking health care. In May 2025, UNFPA estimated 14,800 pregnant women in the West Bank faced limited or no care, and over 1,600 births were expected to take place in unsafe conditions. Nearly 1,000 Israeli checkpoints, gates, and roadblocks have made access to essential services nearly impossible.“The army barely allows us to breathe”, says Haneen, (pictured below right) a mother of three who has walked for two hours to reach a clinic.Hiba knows all too well that these barriers don’t just cost time, they cost lives: “A few months ago, I lost my baby son at four months old…He was the boy I always prayed for,” she said. “But we had no clinic here, and no way to get to one in time. I waited for hours for a ride. He didn’t make it.” In the face of escalating conflict and ever-tightening restrictions on movement, in 2024 PFPPA took their life-saving services to those women cut off from care. Travelling to some of the most hard-to-reach areas, their mobile clinics contain laboratory equipment, ultrasound devices and medication which would otherwise be inaccessible or unaffordable for most of the women in these communities.“Reaching remote villages is never easy - blocked roads, settler threats, or sudden orders to turn back are constant, but we try,” said Dr. Ghada, (pictured above left) a gynaecologist and obstetrician for 15 years. “Every woman deserves care.” Shayma, 22, visited a mobile clinic for a check up as her two children waited nearby:“We’re under serious economic pressure since this war started. Unemployment is up, and movement restrictions make everything harder.” Alongside maternity care, the clinics also provide wider sexual and reproductive health care, including care and advice around contraception and support related to gender-based violence. Kifah, (pictured below) 37, mother of six and an Islamic Studies graduate, knows that knowledge is power - even in crisis.“I’ve been putting myself last,” she said, describing months of delays in seeking gynaecological care. Checkpoints, settler threats, and fear have kept her confined. “Family planning is part of self-care. It’s a right, and it’s responsible, especially now.” She shares this message with other women in her village, telling them that caring for themselves and their reproductive health is an act of strength.Aya, 23, is a mother of two who remembers a neighbour forced to give birth at a checkpoint. She hopes to get an IUD to avoid an unintended pregnancy. “I can’t bring another child into this and tell them I can’t even afford a toy,” she said. So far, these mobile clinics have provided over 60,000 medical services to more than 10,000 people that may otherwise have received no sexual and reproductive healthcare. As well as the clinics, with funding from the Japan Supplementary Budget (JSB), PFPPA have also run ‘preparing for birth’ sessions, midwifery home visits, and community-based awareness sessions around safe childbirth and reproductive health. Maysa Shalaldeh (pictured above left) is an experienced psycho-social worker and the Gender Focal Person in PFPPA, delivering gender-based violence related services for women. Born and raised in Hebron, she is clear about the layered challenges Palestinian women face: legal discrimination, social stigma, economic pressure, and military occupation:“We can’t talk about rights with someone who’s struggling to afford food,” she says. “We meet people where they are. In some places, we start with nutrition or hygiene. In others, we talk about safety or mobility. Then, when there’s trust, we talk about family planning or empowerment. They are survivors. They are women with strength and dignity, navigating unimaginable hardship.”Determined, courageous women like Maysa are the cornerstone of PFPPA’s work - from social workers and pharmacists to doctors and health workers. A nurse with nearly 20 years of experience, Lubna (pictured above right) works at the mobile clinics, helping women feel safe and heard, and guiding them through their options:“I keep learning about reproductive health because I want to empower others. We live in a society where women always put themselves last. I try to show them: we put you first, because you matter.” Shaima, 27, a pharmacist with PFPPA, lights up when talking about her work. “This is the most meaningful part of my job - reaching women we’d never reach otherwise,” she said. In remote villages, she distributes medication and offers advice, but also something less tangible: trust. “I feel proud every time a woman asks me a question she was afraid to ask before,” she says. “They need more than medicine - they need someone who listens.” The work of these women has inspired others to learn and share their knowledge within their communities. Aida, (pictured above) is a mother of six and a community leader. After joining training sessions with PFPPA in reproductive health, she now volunteers with her local women’s association to share her knowledge:“We need each other more than ever. These pressures keep us from making the decisions we need. We have to lift each other up.” For women like Hiba, still reeling from the loss of her young baby, and facing the terrifying prospect of giving birth again without medical care, PFPPA’s support is a lifeline. And, along with the hundreds of women who walk through the doors of their mobile clinics, she demands a safer future for herself and her family:“I have to believe there’s a better world waiting. For my girls. For this baby. Freedom is not worrying about checkpoints. It’s giving birth safely. It’s walking to a clinic without fear. Family planning is wise. It’s power. We women need to be heard. We know what’s best for our bodies and our families.”Her words echo the determination of thousands of Palestinian women - patients, doctors, midwives, psychologists, and volunteers - who continue to protect one another’s health and dignity despite the barriers around them. Their work is not only care - it is resistance, resilience, and hope. This work was made possible thanks to generous funding from the Government of Japan.
SALAMA Concludes Japan-Funded Project to Strengthen Maternal and Reproductive Health for Vulnerable Communities in Lebanon
Beirut, Lebanon - The Lebanese Association for Family Health (SALAMA)—IPPF’s Member Association in Lebanon—hosted the closing ceremony of its Japan-funded project, “Preventing Maternal and Reproductive Health Morbidities and Mortalities among Crisis-Affected Populations, IDPs, Syrian Refugees, and Host Communities in Lebanon,” in Beirut, in the presence of a panel of participants, including the representatives of the Lebanese Ministries of Health and Social Affairs, the Government of Japan, and the IPPF.Funded through the Japan Supplementary Budget (JSB) 2024, the initiative has significantly enhanced access to lifesaving maternal and sexual and reproductive health (SRH) services for crisis-affected communities in Lebanon’s Bekaa Valley, including internally displaced persons (IDPs), Syrian refugees, and host communities.Project Achievements:85,684 SRH services delivered, reaching 28,562 beneficiaries.5,836 women received comprehensive maternal, newborn, and child health care.134 safe deliveries supported through partner hospitals.Sustained operation of two SALAMA clinics in the Bekaa Valley.Community outreach reached 5,960 individuals, with 200 mama-baby kits and 3,000 dignity kits distributed.Capacity-building trainings strengthened healthcare providers’ skills, while partnerships with municipalities and humanitarian actors ensured wider outreach and sustainability.Since 2017, Lebanon has faced overlapping crises—including economic collapse, the Beirut Port explosion, and regional conflicts—that have placed immense strain on its healthcare system. Vulnerable populations, particularly women, girls, IDPs, and refugees, have been disproportionately affected.With the generous support of the Government of Japan, SALAMA has implemented three humanitarian projects funded through the Japan Trust Fund (JTF) and JSB, delivering over 196,441 SRH services in the Bekaa Valley. These interventions have strengthened community resilience, ensured continuity of lifesaving services during prolonged crises, and integrated SRH, mental health, and gender-based violence (GBV) services through structured referral mechanisms. “The completion of this vital project in the Bekaa Valley exemplifies Japan’s steadfast commitment to protecting Sexual and Reproductive Health and Rights,” said Japan’s Ambassador to Lebanon, H.E. Kenji Yokota. “Beyond the provision of essential medical services, it upholds the fundamental right of every individual to live with dignity. This initiative embodies our Human Security approach by empowering individuals and ensuring that no one is left behind,” he added. “Japan remains dedicated to standing alongside Lebanon in supporting resilience, recovery, and long-term stability," he stressed.“From our very first steps, the Government and people of Japan have stood beside SALAMA, enabling us to serve and empower communities through years of crisis,” said Lina Sabra, Executive Director of SALAMA. “Their support, particularly in this recent project, has been a lifeline for families rebuilding after conflict. We are deeply grateful for this enduring partnership.”Through these initiatives, SALAMA has reinforced human security by protecting vulnerable individuals from disease, violence, and psychological distress, while empowering them to make informed decisions about their health and strengthening solidarity within families, communities, and health systems.About SALAMAThe Lebanese Association for Family Health “SALAMA” was founded in 2008. It is a member association of the International Planned Parenthood Federation (IPPF) which is the largest voluntary non-governmental organization in the world, working on sexual and reproductive health and rights (SRHR) issues and advocating for them. SALAMA promotes and provides high quality services, and raises awareness for all groups in the society, particularly the under-served and marginalized.About IPPFThe International Planned Parenthood Federation (IPPF) is a global federation of more than 100 locally led Member Associations working in over 150 countries to advance sexual and reproductive health and rights. In humanitarian settings, IPPF plays a critical role in delivering lifesaving maternal, sexual and reproductive health services to crisis-affected communities, including displaced populations and those facing conflict, disaster, and instability. Through its locally rooted Member Associations, IPPF provides frontline health care, supports preparedness and emergency response, strengthens health systems, and advocates for the protection of rights and dignity in even the most challenging contexts. Locally led and globally connected, IPPF combines service delivery, policy advocacy, and community engagement to ensure that no one is left behind, particularly those most underserved in humanitarian crises.
10 December 2025
Connecting Survivors to Care: A Multi-Layered Sexual and Gender-Based Violence Humanitarian Response in Sudan
The last two years of war between the Sudanese Armed Force and Rapid Support Forces have displaced over 10 million people in Khartoum, the nation’s capital, alongside regions like Darfur and Al Jazirah state. Half of the population is estimated to face acute food insecurity and there have been over 600 attacks on healthcare personnel since April 15 2023, with four attacks on healthcare facilities in January 2025. While recent statistics on maternal and reproductive health have been largely unavailable due to the conflict, maternal mortality in Sudan was among the highest in the world prior to April 2023 and access to quality sexual and reproductive healthcare has been impeded by displacement-related loss of healthcare personnel. Access to SRH services has been further impeded by stockouts of essential medicines such as emergency contraception, injectable long-acting contraception, and antibiotics for sexually transmitted infections.Despite widespread underreporting of SGBV due to cultural stigma, there are indications that sexual violence has been weaponized as an act of war. In Al Jazirah state, government officials have reported 890 cases of rape perpetrated by RSF members, resulting in 125 unwanted pregnancies. In some cases, sexual violence has resulted in severe injury and death. Women have reported both suicidal ideation and attempt after experiencing sexual violence. The actual numbers are expected to be much higher than what was recorded. Indeed, most cases and stories have gone untold; women’s rights activists estimate that only 2% of cases are reported in Sudan, and globally only 1% of adolescent girls seek help after experiencing sexual violence.In addition to risks of sexual violence as a weapon of war by armed groups, internally displaced women face sexual exploitation within temporary resettlement and camp sites. School buildings and other facilities have been repurposed to house displaced families and there are often over ten people residing together from multiple families within the same room. In this context, there is no privacy, and these risks to women are compounded within host communities, where women often receive threats as they leave IDP sites to look for work or to purchase needed resources for their families.In this context of amplified risks of SGBV and unmet need for healthcare services, the Sudanese Family Planning Association has worked with partner organizations to provide comprehensive care to SGBV survivors and has utilized social media to raise awareness about SGBV and available services for survivors. SFPA operates a four-pronged approach to addressing SGBV. Through a combination of direct clinical service points, partnerships and coordination with other NGOs, group-based discussions and individual home visits, SRH hotline, and social media strategy, the organization has been connecting survivors to care, providing medical services and referrals, and raising awareness and challenging stigmatization of SGBV.SFPA operates 26 static clinics and has used multiple mechanisms to provide services across the development-humanitarian nexus. Through 39 mobile service delivery team deployments to reach IDP camps, SFPA reached over 20,000 people displaced by conflict in Umrakoba & Tunaydbah between June and November 2024. In addition to directly providing clinical SRH and SGBV services, mobile service delivery teams shared information about SGBV to 4,506 individuals through a combination of 1499 group-level awareness raising sessions in clinic waiting areas and home visits to assess health needs on a more confidential basis. Female youth attending group-based sessions in Umrakoba & Tunaydbah shared that they gained awareness about their rights and referral pathways for violence, and adult women reported that they learned strategies for protecting and listening to their children. At these first points of in-person contact, staff have received a number of SGBV disclosures and referred survivors to clinical services.In addition to clinical services and in-person awareness-raising activities, SFPA has supported comprehensive care through coordination and partnerships with local and international NGOs. Survivors of sexual and gender-based violence must navigate a complex legal terrain as abortion is a crime in Sudan, only legally permissible in cases of rape, threats to the pregnant woman’s life, and foetal death within the womb. Women who become pregnant due to rape need police permission to undergo an abortion. In cases of pregnancy due to rape, partner organization Mutawinat obtains permission from police offices to provide abortion and SFPA directly performs the abortion for clients. SFPA also partners with an organization which provides shelter for women who become pregnant to ensure shelter and care through birth, and another organization provides financial support after birth. SFPA has also expanded access to care through implementation of a call center, or hotline, for SGBV. The call center directly serves survivors through a hotline which connects them to an integrated care team comprised of an obstetrician, family planning providers, and psychosocial support counsellors. By calling a central number – 1700 – survivors can share information about their needs and connect to available services. In 2024, the hotline received a total of 79,900 calls and provided 1,544,297 digital services. SFPA provided 2,331 SGBV services, and 60% of digitally referred SGBV cases were followed up through health service delivery points. As the war intensified and over 50% of healthcare facilities closed in conflict-affected areas, the hotline became a lifeline for accessing health care, and 45.1% (696,186) of digital services were provided for non-SRH issues.These services are complemented by a social media-based SGBV awareness strategy, implemented by youth workers connected to each SFPA branch. Through social media outlets such as TikTok, Facebook, and WhatsApp, SFPA has reached over 500,000 community members with information on SRHR and SGBV and challenging stigmatization of survivors. Youth workers have created virtual contests and games which have resulted in increasing engagement over time, with 37,000 interactions via Facebook alone.SFPA’s social media strategy has yielded a surprising result: survivors have directly responded to campaigns implemented through outlets to seek resources for support. Social media posts have shared information about SFPA’s hotline and comms staff have provided referrals to clinical services. The organization identified 5,193 clients seeking SRH services through social media outreach, including for SGBV. SFPA’s Dr Limiaa Khalfalla noted the importance of handling such disclosures carefully and ensuring adequate training to protect confidentiality. The call center has been an essential service in responding to these disclosures as a central point of referral where survivors can readily access trained staff. Through IPPF’s STREAM3 funding, SFPA has trained ten employees and eighteen volunteers on topics such as SGBV fundamentals, the LIVES approach, clinical management of rape, and long-acting contraceptive methods.
09 December 2025
Under Siege and Out of Reach: Health, Safety, and Dignity in Sudan
For more than 18 months, el-Fasher has been under siege. Families who once fled to this city in North Darfur for safety are now trapped in it. Around 260,000 civilians – including 130,000 children – are trapped with almost no aid. Food prices have soared, water is unsafe, and bombardment is constant. Those who manage to escape towards Tawila face attacks and extortion on the road. For women and girls, every stage of this journey, staying, fleeing, or arriving in displacement sites, comes with overwhelming, life-threatening risks. Across Sudan, the war between the Sudanese Armed Forces and the Rapid Support Forces (RSF) has driven one of the world’s fastest-growing displacement and hunger crises. Starvation is being used as a tactic of war, with el-Fasher a stark example. The scale of atrocities have drawn the attention of UN genocide prevention experts, and all the while, devastation spreads like wildfire. Within this wider collapse, the sexual and reproductive health and rights (SRHR) of women and girls are being systematically eroded. Gendered violence and SRHR under siegeWomen and girls in el-Fasher describe life under siege as “death by missiles, starvation and daily violations”. Families are surviving on animal feed and leaves. Girls often eat last and least, if at all. Malnutrition is rising sharply among pregnant women, new mothers and young children, heightening risks of maternal death, unsafe childbirth, and child and infant deaths. Conflict-related sexual violence has surged. Reports from el-Fasher and surrounding areas point to horrific crimes of abduction for ransom, sexual assault, and captivity as civilians attempt to move in or out of the city. Young people are particularly exposed, both during flight and in overcrowded camps where lighting, privacy and safe WASH facilities are scarce. Access to post-rape care – including emergency contraception, HIV prophylaxis, safe abortion, and psychosocial support – is extremely limited. The health system that should protect women’s lives has itself become a target. In October, armed men attacked Saudi Maternity Hospital, the only partially functioning hospital left in el-Fasher at the time. More than 460 patients and their companions were reportedly killed, and six health workers abducted, in what the World Health Organization has condemned as a flagrant attack on health care. Many of those killed and injured were women in labour and newborns. This is not an isolated incident. Clinics have been looted or destroyed, staff have fled or been killed, and basic supplies, from blood bags to oxytocin, have run out. The result is that women are giving birth at home, on the road, or in makeshift shelters without skilled care. Complications that should be easily managed are becoming fatal. At the same time, contraceptive stocks are depleted, increasing the risk of unintended pregnancies in a context of extreme violence and hunger. UN Women, UNFPA, WHO and others have documented how these patterns are not accidental but part of a broader assault on women’s rights and bodily autonomy in Sudan. Together they amount to a major rollback of SRHR gains achieved over decades, and a direct attack on the core of the Women, Peace and Security agenda. The WPS agenda recognises that women are disproportionately affected by conflict and must be given space to actively participate, be heard and represented in all peace and security processes. You can read more in UN Women’s explainer on the WPS agenda and in our factsheet on why SRHR must be part of WPS. Women are being targeted – and often the first to respondWhile formal systems collapse, Sudanese women’s organisations and health workers are holding the line. Local groups in conflict-ridden contexts have set up communal kitchens, organised food sharing, and identified malnourished children and pregnant women most in need of support. They provide information on contraception, support survivors of violence, and coordinate safe spaces in displacement camps. These are not external actors parachuting in; they are women from affected communities, doing protection and relief work often without pay or protection. Sexual and reproductive health services are still being provided in some areas by midwives, nurses and doctors working with Sudanese organisations, UN agencies and international NGOs. UNFPA and partners have supported emergency obstetric and newborn care in sites like Tawila, where many of those fleeing el-Fasher arrive. But insecurity and funding gaps mean these services reach only a fraction of those who need them. The Sudan Family Planning Association (SFPA), member association of IPPF in Sudan, has been at the forefront of this work. End of October, SFPA reported that one staff member has been detained and nine others remain missing after targeted attacks in el-Fasher; several of its clinics have been destroyed. SFPA had helped to improve Saudi Maternity Hospital’s capacities prior to the October massacre. Despite the loss of colleagues, facilities and equipment, SFPA and IPPF continue to provide SRHR services where they can – often through mobile teams and community networks – and to call for protection of health workers and facilities. This is the Women, Peace and Security (WPS) agenda in practice: women not only experiencing the worst impacts of conflict, but also at the front of humanitarian response, sustaining communities and demanding accountability. Yet they remain largely excluded from formal decision-making on ceasefires, humanitarian access and the future of Sudan. What Europe and the wider international community must doThe situation in el-Fasher is not only a humanitarian emergency; it is a test of whether governments will uphold their commitments on SRHR, international humanitarian law, and the WPS agenda during political strife. We are calling for urgent, concrete steps: Put SRHR at the centre of the humanitarian response. The EU and European governments should increase flexible humanitarian funding for Sudan, explicitly earmarking support for SRHR: emergency obstetric and newborn care, contraception, safe abortion care, and comprehensive clinical and psychosocial services for survivors of sexual violence. Funding must reach frontline providers – including SFPA, women-led organisations and community health workers.Protect women, girls and health workers. All parties to the conflict must immediately cease attacks on civilians, health facilities and humanitarian workers, in line with international humanitarian and human rights law. European governments should press for international investigations into attacks such as the Saudi Maternity Hospital massacre, and support mechanisms to document, prosecute and sanction those responsible for conflict-related sexual violence and attacks on health care. Open safe, monitored humanitarian corridors. The EU and Member States should use diplomatic and political leverage – including within the UN Security Council and regional forums – to secure a sustained ceasefire around el-Fasher and other besieged areas, and guarantee safe, unimpeded humanitarian access by land. Any “humanitarian corridor” must be genuinely safe, including for women, girls and other at-risk groups, and monitored by neutral actors.Back women’s leadership and participation. Women’s rights organisations, including those working on SRHR, must be funded and recognised as essential humanitarian and peacebuilding actors, not as add-ons. European support should enable Sudanese women peacebuilders, health workers and activists to participate meaningfully in ceasefire talks, political negotiations and reconstruction planning, in line with the WPS agenda.Sustain long-term SRHR and gender equality funding. Beyond immediate relief, the EU and European governments should protect and expand development and SRHR funding for Sudan and the region, avoiding cuts or reallocation that would further weaken fragile health systems. Investments should support comprehensive SRHR services, maternal and newborn health, adolescent girls’ health and education, and community-based work to prevent and respond to gender-based violence, including harmful practices such as FGM. The war in Sudan, the siege of el-Fasher in particular, is exposing just how quickly women’s and girls’ rights can be dismantled when conflict, impunity and neglect converge. It is also showing, once again, that women are central to any meaningful response. In this devastating situation, we are calling on European countries and the European Union to take urgent action to uphold the rights, health, and dignity of Sudanese people. This article was originally published on countdown2030Europe.
IPPF stands against Trumps enforced silence on World AIDS Day
This year, the Trump administration has banned federal employees and grant recipients from acknowledging World AIDS Day, celebrated on the 1st December 2025. The State Department’s directive told employees to “refrain from publicly promoting World AIDS Day through any communication channels, including social media, media engagements, speeches or other public-facing messaging”.This latest directive comes after US funding cuts this year put essential sexual and reproductive healthcare, which includes HIV prevention services, at risk for millions worldwide. A global survey of Member Associations conducted by IPPF revealed the devastating impacts on our Member Associations who provide integrated sexual and reproductive healthcare services. Over half our Member Associations were affected, with an estimated loss of $85million. The Trump administration’s decision to enforce silence around World AIDS Day demonstrates a lack of respect for the lived experiences of those living with HIV, those who died of AIDS, and all affected by HIV. This directive impedes the ongoing efforts to reduce the transmission of HIV and to address stigma, discrimination, and inequality. These decisions are not isolated from broader state driven ideologies and anti-rights pushbacks that continue to suppress the acceptance and fair inclusion of all people in society. This enforced silence on World AIDS Day serves only to further embed stigma and injustice and is another reminder as to why we must confront these moments with equal strength and clarity. IPPF supports the rights of all people in society and works to provide sexual and reproductive health services to all, in particular those who are marginalised, such as gay men and other men who have sex with men, sex workers, trans people, people who inject drugs, and prisoners. IPPF works with our Member Associations doing vital work to support those living with HIV, to end stigma, and ‘overcome disruption’ to providing essential health services to communities, including HIV testing, prevention and treatment. In times of crisis and oppression, rights and dignity need champions. At IPPF we carry this moment with our Member Associations on the ground and stand behind them in their continued dignity and fight for the right to continue the vital work they do. At IPPF we will continue our work towards a vision of a world free from HIV where everyone is valued equally, has a healthy, pleasurable, and fulfilling life within a just and equal society. Key to an impactful HIV programme is understanding and addressing drivers of the HIV pandemic, including structural barriers; violence against women; discrimination; stigma; harmful social norms; inequalities related to sex, gender, sexual orientation, race, disability, and economic status; criminalisation of HIV transmission and certain populations; and restrictive laws and policies.Due to social and biological vulnerabilities, certain groups of people experience higher rates of HIV including women and girls; gay, bisexual, and other men who have sex with men; sex workers; people who inject drugs; trans people; and people in prisons. Working with those affected by and living with HIV to design, implement, and evaluate IPPF services and programmes is essential on our pathway to realise a society free of discrimination and stigma, and for all people living with HIV to live healthy and fulfilled lives. A community-led and inclusive response includes both tailoring services and programmes to address the needs of communities more severely affected by HIV, as well as addressing the needs of all people who would benefit from HIV‑related services such as youth, people with disabilities, pregnant women and infants, people in sexual relationships with individuals living with HIV, boys and men, and others who may not identify as a member of certain groups. Of key importance is creating programmes, services, and spaces that are inclusive, discrimination-free, and accessible to all, where each person feels welcomed and that their health and well‑being needs will be at the centre of the care that they receive.At IPPF our Member Association’s work demonstrates what we can achieve when we lead with community-led responses. For example, in Mozambique, the Associação Moçambicana para o Desenvolvimento da Família (AMODEFA), together with sex workers, are working to ensure that sex workers have access to comprehensive sexual and reproductive health services, with oral pre-exposure prophylaxis (PrEP*) for HIV prevention.In Zambia, the Planned Parenthood Association of Zambia (PPAZ), through a partnership between the Children’s Investment Fund Foundation (CIFF) and the Global Fund to Fight AIDS, Tuberculosis, and Malaria—has secured 21,600 Dapivirine Vaginal Rings for HIV prevention for women. Adding the PrEP ring as an additional HIV prevention option gives women more choice about which HIV prevention method they can use, empowers them to make informed decisions about their health, and increases the chance that individuals can find a method that works for them.On Worlds AIDS day we are doubling down on our commitment and support to the communities we work with and our Member Associations who continue to provide innovative healthcare models to prevent HIV transmission, and provide vital care to those living with HIV. The work in Mozambique and Zambia are just two examples of the work that many Member Associations are implementing globally to provide essential health services to communities, including HIV testing, treatment and prevention. *Pre-Exposure Prophylaxis (PrEP) is used to reduce the risk of getting HIV.